
Page 175 - Read Online
P. 175
Borzio et al. Hepatoma Res 2019;5:15 I http://dx.doi.org/10.20517/2394-5079.2019.11 Page 3 of 16
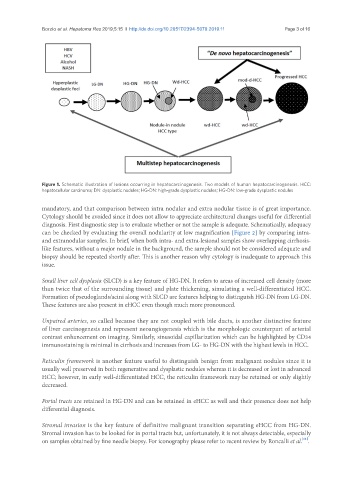
Figure 1. Schematic illustration of lesions occurring in hepatocarcinogenesis. Two models of human hepatocarcinogenesis. HCC:
hepatocellular carcinoma; DN: dysplastic nodules; HG-DN: high-grade dysplastic nodules; HG-DN: low-grade dysplastic nodules
mandatory, and that comparison between intra nodular and extra nodular tissue is of great importance.
Cytology should be avoided since it does not allow to appreciate architectural changes useful for differential
diagnosis. First diagnostic step is to evaluate whether or not the sample is adequate. Schematically, adequacy
can be checked by evaluating the overall nodularity at low magnification [Figure 2] by comparing intra-
and extranodular samples. In brief, when both intra- and extra-lesional samples show overlapping cirrhosis-
like features, without a major nodule in the background, the sample should not be considered adequate and
biopsy should be repeated shortly after. This is another reason why cytology is inadequate to approach this
issue.
Small liver cell dysplasia (SLCD) is a key feature of HG-DN. It refers to areas of increased cell density (more
than twice that of the surrounding tissue) and plate thickening, simulating a well-differentiated HCC.
Formation of pseudoglands/acini along with SLCD are features helping to distinguish HG-DN from LG-DN.
These features are also present in eHCC even though much more pronounced.
Unpaired arteries, so called because they are not coupled with bile ducts, is another distinctive feature
of liver carcinogenesis and represent neoangiogenesis which is the morphologic counterpart of arterial
contrast enhancement on imaging. Similarly, sinusoidal capillarization which can be highlighted by CD34
immunostaining is minimal in cirrhosis and increases from LG- to HG-DN with the highest levels in HCC.
Reticulin framework is another feature useful to distinguish benign from malignant nodules since it is
usually well preserved in both regenerative and dysplastic nodules whereas it is decreased or lost in advanced
HCC; however, in early well-differentiated HCC, the reticulin framework may be retained or only slightly
decreased.
Portal tracts are retained in HG-DN and can be retained in eHCC as well and their presence does not help
differential diagnosis.
Stromal invasion is the key feature of definitive malignant transition separating eHCC from HG-DN.
Stromal invasion has to be looked for in portal tracts but, unfortunately, it is not always detectable, especially
[11]
on samples obtained by fine needle biopsy. For iconography please refer to recent review by Roncalli et al. .