
Page 20 - Read Online
P. 20
Nishioka et al. Hepatoma Res 2018;4:1 I http://dx.doi.org/10.20517/2394-5079.2017.46 Page 9 of 12
A Product-limit survival estimates B Product-limit survival estimates
1.0 + Censored 1.0 + Censored
0.8
Survival probability 0.6 Survival probability 0.8
0.6
0.4
0.4
0.2
0.0 0.2
0.0
0 500 1000 1500 2000 0 500 1000 1500 2000
Survival Survival
AFP_GE_400 No Yes Collapsed_Gene_Set S1/S2 S3
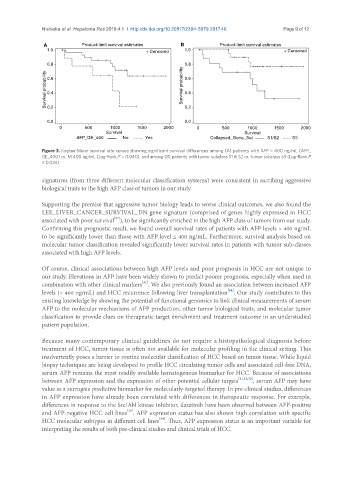
Figure 3. Kaplan-Meier survival rate curves showing significant survival differences among (A) patients with AFP > 400 ng/mL (AFP_
GE_400) vs. ≤ 400 ng/mL (Log-Rank P = 0.040), and among (B) patients with tumor subclass S1 & S2 vs. tumor subclass S3 (Log-Rank P
= 0.024)
signatures (from three different molecular classification systems) were consistent in ascribing aggressive
biological traits to the high AFP class of tumors in our study.
Supporting the premise that aggressive tumor biology leads to worse clinical outcomes, we also found the
LEE_LIVER_CANCER_SURVIVAL_DN gene signature (comprised of genes highly expressed in HCC
[27]
associated with poor survival ), to be significantly enriched in the high AFP class of tumors from our study.
Confirming this prognostic result, we found overall survival rates of patients with AFP levels > 400 ng/mL
to be significantly lower than those with AFP level ≤ 400 ng/mL. Furthermore, survival analysis based on
molecular tumor classification revealed significantly lower survival rates in patients with tumor sub-classes
associated with high AFP levels.
Of course, clinical associations between high AFP levels and poor prognosis in HCC are not unique to
our study. Elevations in AFP have been widely shown to predict poorer prognosis, especially when used in
[31]
combination with other clinical markers . We also previously found an association between increased AFP
[24]
levels (> 400 ng/mL) and HCC recurrence following liver transplantation . Our study contributes to this
existing knowledge by showing the potential of functional genomics to link clinical measurements of serum
AFP to the molecular mechanisms of AFP production, other tumor biological traits, and molecular tumor
classification to provide clues on therapeutic target enrichment and treatment outcome in an understudied
patient population.
Because many contemporary clinical guidelines do not require a histopathological diagnosis before
treatment of HCC, tumor tissue is often not available for molecular profiling in the clinical setting. This
inadvertently poses a barrier to routine molecular classification of HCC based on tumor tissue. While liquid
biopsy techniques are being developed to profile HCC circulating tumor cells and associated cell-free DNA,
serum AFP remains the most readily available hematogenous biomarker for HCC. Because of associations
between AFP expression and the expression of other potential cellular targets [11,12,32] , serum AFP may have
value as a surrogate predictive biomarker for molecularly-targeted therapy. In pre-clinical studies, differences
in AFP expression have already been correlated with differences in therapeutic response. For example,
differences in response to the Src/Abl kinase inhibitor, dasatinib have been observed between AFP-positive
and AFP-negative HCC cell lines . AFP expression status has also shown high correlation with specific
[33]
[34]
HCC molecular subtypes in different cell lines . Thus, AFP expression status is an important variable for
interpreting the results of both pre-clinical studies and clinical trials of HCC.