
Page 69 - Read Online
P. 69
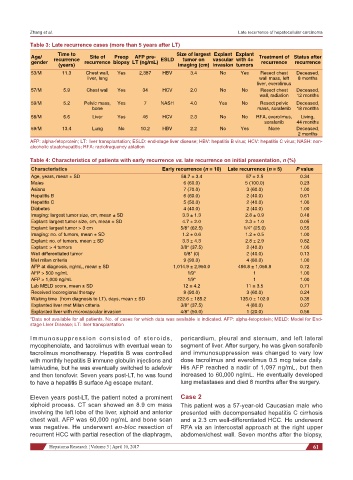
Zhang et al. Late recurrence of hepatocellular carcinoma
Table 3: Late recurrence cases (more than 5 years after LT)
Age/ Time to Site of Preop AFP pre- Size of largest Explant Explant Treatment of Status after
tumor on
gender recurrence recurrence biopsy LT (ng/mL) ESLD imaging (cm) vascular with 4+ recurrence recurrence
tumors
invasion
(years)
53/M 11.3 Chest wall, Yes 2,387 HBV 3.4 No Yes Resect chest Deceased,
liver, lung wall mass, left 8 months
liver, everolimus
57/M 5.9 Chest wall Yes 34 HCV 2.0 No No Resect chest Deceased,
wall, radiation 12 months
59/M 5.2 Pelvic mass, Yes 7 NASH 4.0 Yes No Resect pelvic Deceased,
bone mass, sorafenib 18 months
58/M 6.6 Liver Yes 46 HCV 2.3 No No RFA, everolimus, Living,
sorafenib 44 months
59/M 13.4 Lung No 10.2 HBV 2.2 No Yes None Deceased,
2 months
AFP: alpha-fetoprotein; LT: liver transplantation; ESLD: end-stage liver disease; HBV: hepatitis B virus; HCV: hepatitis C virus; NASH: non-
alcoholic steatohepatitis; RFA: radiofrequency ablation
Table 4: Characteristics of patients with early recurrence vs. late recurrence on initial presentation, n (%)
Characteristics Early recurrence (n = 10) Late recurrence (n = 5) P value
Age, years, mean ± SD 58.7 ± 3.4 57 ± 2.5 0.34
Males 6 (60.0) 5 (100.0) 0.23
Asians 7 (70.0) 3 (60.0) 1.00
Hepatitis B 6 (60.0) 2 (40.0) 0.61
Hepatitis C 5 (50.0) 2 (40.0) 1.00
Diabetes 4 (40.0) 2 (40.0) 1.00
Imaging: largest tumor size, cm, mean ± SD 3.3 ± 1.3 2.8 ± 0.9 0.48
Explant: largest tumor size, cm, mean ± SD 4.7 ± 2.0 2.3 ± 1.0 0.05
Explant: largest tumor > 3 cm 5/8* (62.5) 1/4* (25.0) 0.55
Imaging: no. of tumors, mean ± SD 1.2 ± 0.6 1.2 ± 0.5 1.00
Explant: no. of tumors, mean ± SD 3.3 ± 4.3 2.8 ± 2.9 0.82
Explant: > 4 tumors 3/8* (37.5) 2 (40.0) 1.00
Well differentiated tumor 0/8* (0) 2 (40.0) 0.13
Met milan criteria 9 (90.0) 4 (80.0) 1.00
AFP at diagnosis, ng/mL, mean ± SD 1,014.9 ± 2,950.0 496.8 ± 1,056.8 0.72
AFP > 500 ng/mL 1/9* 1 1.00
AFP > 1,000 ng/mL 1/9* 1 1.00
Lab MELD score, mean ± SD 12 ± 4.2 11 ± 3.5 0.71
Received locoregional therapy 9 (90.0) 3 (60.0) 0.24
Waiting time (from diagnosis to LT), days, mean ± SD 222.6 ± 185.2 135.0 ± 102.0 0.35
Explanted liver met Milan criteria 3/8* (37.5) 4 (80.0) 0.27
Explanted liver with microvascular invasion 4/8* (50.0) 1 (20.0) 0.56
*Data not available for all patients. No. of cases for which data was available is indicated. AFP: alpha-fetoprotein; MELD: Model for End-
stage Liver Disease; LT: liver transplantation
Immunosuppression consisted of steroids, pericardium, pleural and sternum, and left lateral
mycophenolate, and tacrolimus with eventual wean to segment of liver. After surgery, he was given sorafenib
tacrolimus monotherapy. Hepatitis B was controlled and immunosuppression was changed to very low
with monthly hepatitis B immune globulin injections and dose tacrolimus and everolimus 0.5 mcg twice daily.
lamivudine, but he was eventually switched to adefovir His AFP reached a nadir of 1,097 ng/mL, but then
and then tenofovir. Seven years post-LT, he was found increased to 60,000 ng/mL. He eventually developed
to have a hepatitis B surface Ag escape mutant. lung metastases and died 8 months after the surgery.
Eleven years post-LT, the patient noted a prominent Case 2
xiphoid process. CT scan showed an 8.9 cm mass This patient was a 57-year-old Caucasian male who
involving the left lobe of the liver, xiphoid and anterior presented with decompensated hepatitis C cirrhosis
chest wall. AFP was 60,000 ng/mL and bone scan and a 2.3 cm well-differentiated HCC. He underwent
was negative. He underwent en-bloc resection of RFA via an intercostal approach at the right upper
recurrent HCC with partial resection of the diaphragm, abdomen/chest wall. Seven months after the biopsy,
Hepatoma Research ¦ Volume 3 ¦ April 10, 2017 61