
Page 63 - Read Online
P. 63
Hung et al. Attenuation of liver stiffness by sorafenib
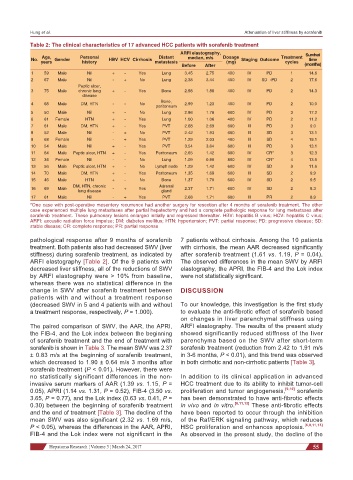
Table 2: The clinical characteristics of 17 advanced HCC patients with sorafenib treatment
ARFI elastography,
Age, Personal Distant median, m/s Dosage Treatment Survival
No. Gender HBV HCV Cirrhosis Staging Outcome time
years history metastasis (mg) cycles
Before After (months)
1 59 Male Nil + - Yes Lung 3.45 2.75 400 IV PD 1 14.6
2 67 Male Nil - + No Lung 2.38 3.44 400 IV SD→PD 2 17.6
Peptic ulcer,
3 75 Male chronic lung + - Yes Bone 2.98 1.88 400 IV PD 2 14.3
disease
Bone,
4 68 Male DM, HTN - - No 2.99 1.23 400 IV PD 2 10.0
peritoneum
5 50 Male Nil + - No Lung 2.86 1.78 600 IV PD 3 17.2
6 61 Female HTN + - Yes Lung 1.00 1.06 400 IV PD 2 11.2
7 61 Male DM, HTN + - Yes PVT 2.68 2.69 600 III PD 3 9.0
8 52 Male Nil - + No PVT 2.42 1.93 600 III SD 3 13.1
9 68 Female Nil - + Yes PVT 1.29 2.03 400 III SD 4 19.1
10 54 Male Nil + - Yes PVT 3.54 3.64 600 III PD 3 13.1
11 64 Male Peptic ulcer, HTN + - Yes Peritoneum 2.65 1.42 600 IV CR* 3 12.3
12 34 Female Nil - - No Lung 1.09 0.90 800 IV CR* 4 13.6
13 56 Male Peptic ulcer, HTN + - No Lymph node 1.29 1.42 600 IV SD 3 11.6
14 70 Male DM, HTN + - Yes Peritoneum 1.35 1.69 600 III SD 2 9.9
15 46 Male HTN + - No Bone 1.37 1.70 600 IV SD 2 9.5
DM, HTN, chronic Adrenal
16 69 Male - + Yes 2.37 1.71 600 IV SD 2 8.3
lung disease gland
17 61 Male Nil - + Yes PVT 2.68 1.71 600 III PR 2 8.9
*One case with post-operative mesentery recurrence had another surgery for resection after 4 months of sorafenib treatment. The other
case experienced multiple lung metastases after partial hepatectomy and had a complete pathologic response for lung metastases after
sorafenib treatment. These pulmonary lesions enlarged initially and regressed thereafter. HBV: hepatitis B virus; HCV: hepatitis C virus;
ARFI: acoustic radiation force impulse; DM: diabetes mellitus; HTN: hypertension; PVT: partial response; PD: progressive disease; SD:
stable disease; CR: complete response; PR: partial response
pathological response after 9 months of sorafenib 7 patients without cirrhosis. Among the 10 patients
treatment. Both patients also had decreased SWV (liver with cirrhosis, the mean AAR decreased significantly
stiffness) during sorafenib treatment, as indicated by after sorafenib treatment (1.61 vs. 1.19, P = 0.04).
ARFI elastography [Table 2]. Of the 9 patients with The observed differences in the mean SWV by ARFI
decreased liver stiffness, all of the reductions of SWV elastography, the APRI, the FIB-4 and the Lok index
by ARFI elastography were > 10% from baseline, were not statistically significant.
whereas there was no statistical difference in the
change in SWV after sorafenib treatment between DISCUSSION
patients with and without a treatment response
(decreased SWV in 5 and 4 patients with and without To our knowledge, this investigation is the first study
a treatment response, respectively, P = 1.000). to evaluate the anti-fibrotic effect of sorafenib based
on changes in liver parenchymal stiffness using
The paired comparison of SWV, the AAR, the APRI, ARFI elastography. The results of the present study
the FIB-4, and the Lok index between the beginning showed significantly reduced stiffness of the liver
of sorafenib treatment and the end of treatment with parenchyma based on the SWV after short-term
sorafenib is shown in Table 3. The mean SWV was 2.37 sorafenib treatment (reduction from 2.42 to 1.91 m/s
± 0.83 m/s at the beginning of sorafenib treatment, in 3-6 months, P < 0.01), and this trend was observed
which decreased to 1.90 ± 0.64 m/s 3 months after in both cirrhotic and non-cirrhotic patients [Table 3].
sorafenib treatment (P < 0.01). However, there were
no statistically significant differences in the non- In addition to its clinical application in advanced
invasive serum markers of AAR (1.39 vs. 1.15, P = HCC treatment due to its ability to inhibit tumor-cell
0.05), APRI (1.14 vs. 1.31, P = 0.52), FIB-4 (3.50 vs. proliferation and tumor angiogenesis, [9,10] sorafenib
3.65, P = 0.77), and the Lok index (0.63 vs. 0.41, P = has been demonstrated to have anti-fibrotic effects
0.30) between the beginning of sorafenib treatment in vivo and in vitro. [6,11,13] These anti-fibrotic effects
and the end of treatment [Table 3]. The decline of the have been reported to occur through the inhibition
mean SWV was also significant (2.32 vs. 1.69 m/s, of the Raf/ERK signaling pathway, which reduces
P < 0.05), whereas the differences in the AAR, APRI, HSC proliferation and enhances apoptosis. [6,8,11,13]
FIB-4 and the Lok index were not significant in the As observed in the present study, the decline of the
Hepatoma Research ¦ Volume 3 ¦ March 24, 2017 55