
Page 95 - Read Online
P. 95
Page 4 of 18 Thiruchelvam et al. Hepatoma Res 2021;7:22 I http://dx.doi.org/10.20517/2394-5079.2020.144
A B
C
D
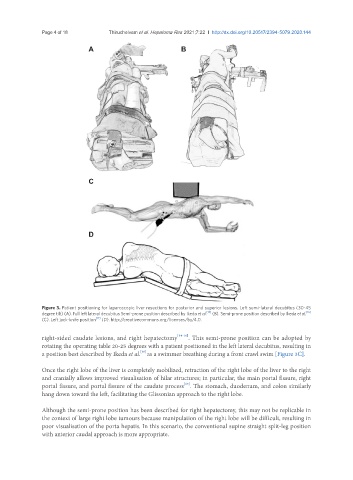
Figure 3. Patient positioning for laparoscopic liver resections for posterior and superior lesions. Left semi-lateral decubitus (30-45
[16]
[15]
degree tilt) (A). Full left lateral decubitus Semi-prone position described by Ikeda et al. (B). Semi-prone position described by Ikeda et al.
(C). Left jack-knife position [17] (D). http://creativecommons.org/licenses/by/4.0.
right-sided caudate lesions, and right hepatectomy [14-16] . This semi-prone position can be adopted by
rotating the operating table 20-25 degrees with a patient positioned in the left lateral decubitus, resulting in
[16]
a position best described by Ikeda et al. as a swimmer breathing during a front crawl swim [Figure 3C].
Once the right lobe of the liver is completely mobilized, retraction of the right lobe of the liver to the right
and cranially allows improved visualisation of hilar structures; in particular, the main portal fissure, right
portal fissure, and portal fissure of the caudate process . The stomach, duodenum, and colon similarly
[15]
hang down toward the left, facilitating the Glissonian approach to the right lobe.
Although the semi-prone position has been described for right hepatectomy, this may not be replicable in
the context of large right lobe tumours because manipulation of the right lobe will be difficult, resulting in
poor visualisation of the porta hepatis. In this scenario, the conventional supine straight split-leg position
with anterior caudal approach is more appropriate.