
Page 87 - Read Online
P. 87
Van Der Steen et al. Cancer Drug Resist 2018;1:230-49 I http://dx.doi.org/10.20517/cdr.2018.13 Page 235
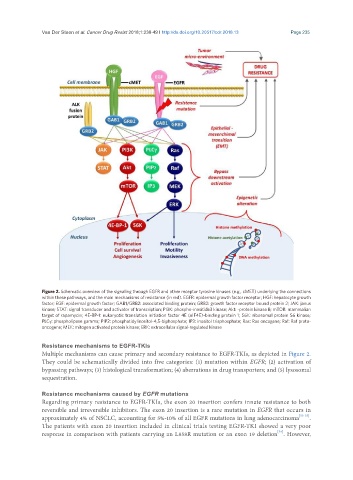
Figure 2. Schematic overview of the signaling through EGFR and other receptor tyrosine kinases (e.g., cMET) underlying the connections
within these pathways, and the main mechanisms of resistance (in red). EGFR: epidermal growth factor receptor; HGF: hepatocyte growth
factor; EGF: epidermal growth factor; GAB1/GRB2: associated binding protein; GRB2: growth factor receptor bound protein 2; JAK: janus
kinase; STAT: signal transducer and activator of transcription; PI3K: phospho-inositide3 kinase; Akt: -protein kinase B; mTOR: mammalian
target of rapamycin; 4E-BP-1: eukaryotic translation initiation factor 4E (eIF4E)-binding protein 1; S6K: ribosomal protein S6 kinase;
PLCγ: phospholipase gamma; PIP2: phosphatidylinositol-4,5-biphosphate; IP3: inositol trisphosphate; Ras: Ras oncogene; Raf: Raf proto-
oncogene; MEK: mitogen activated protein kinase; ERK: extracellular signal-regulated kinase
Resistance mechanisms to EGFR-TKIs
Multiple mechanisms can cause primary and secondary resistance to EGFR-TKIs, as depicted in Figure 2.
They could be schematically divided into five categories: (1) mutation within EGFR; (2) activation of
bypassing pathways; (3) histological transformation; (4) aberrations in drug transporters; and (5) lysosomal
sequestration.
Resistance mechanisms caused by EGFR mutations
Regarding primary resistance to EGFR-TKIs, the exon 20 insertion confers innate resistance to both
reversible and irreversible inhibitors. The exon 20 insertion is a rare mutation in EGFR that occurs in
approximately 4% of NSCLC, accounting for 5%-10% of all EGFR mutations in lung adenocarcinoma [53-55] .
The patients with exon 20 insertion included in clinical trials testing EGFR-TKI showed a very poor
[54]
response in comparison with patients carrying an L858R mutation or an exon 19 deletion . However,