
Page 153 - Read Online
P. 153
Page 220 Grewal et al. Art Int Surg 2023;3:217-32 https://dx.doi.org/10.20517/ais.2023.28
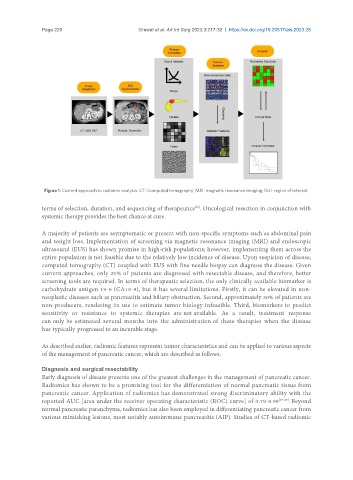
Figure 1. Current approach to radiomic analysis. CT: Computed tomography; MRI: magnetic resonance imaging; ROI: region of interest.
terms of selection, duration, and sequencing of therapeutics . Oncological resection in conjunction with
[26]
systemic therapy provides the best chance at cure.
A majority of patients are asymptomatic or present with non-specific symptoms such as abdominal pain
and weight loss. Implementation of screening via magnetic resonance imaging (MRI) and endoscopic
ultrasound (EUS) has shown promise in high-risk populations; however, implementing them across the
entire population is not feasible due to the relatively low incidence of disease. Upon suspicion of disease,
computed tomography (CT) coupled with EUS with fine needle biopsy can diagnose the disease. Given
current approaches, only 20% of patients are diagnosed with resectable disease, and therefore, better
screening tools are required. In terms of therapeutic selection, the only clinically available biomarker is
carbohydrate antigen 19-9 (CA19-9), but it has several limitations. Firstly, it can be elevated in non-
neoplastic diseases such as pancreatitis and biliary obstruction. Second, approximately 20% of patients are
non-producers, rendering its use to estimate tumor biology infeasible. Third, biomarkers to predict
sensitivity or resistance to systemic therapies are not available. As a result, treatment response
can only be estimated several months into the administration of these therapies when the disease
has typically progressed to an incurable stage.
As described earlier, radiomic features represent tumor characteristics and can be applied to various aspects
of the management of pancreatic cancer, which are described as follows.
Diagnosis and surgical resectability
Early diagnosis of disease presents one of the greatest challenges in the management of pancreatic cancer.
Radiomics has shown to be a promising tool for the differentiation of normal pancreatic tissue from
pancreatic cancer. Application of radiomics has demonstrated strong discriminatory ability with the
reported AUC [area under the receiver operating characteristic (ROC) curve] of 0.79-0.99 [27-29] . Beyond
normal pancreatic parenchyma, radiomics has also been employed in differentiating pancreatic cancer from
various mimicking lesions, most notably autoimmune pancreatitis (AIP). Studies of CT-based radiomic