
Page 44 - Read Online
P. 44
Page 8 of 22 Royse et al. Vessel Plus 2020;4:5 I http://dx.doi.org/10.20517/2574-1209.2019.34
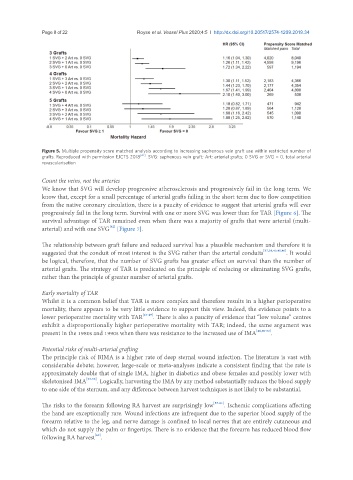
Figure 5. Multiple propensity score matched analysis according to increasing saphenous vein graft use within restricted number of
grafts. Reproduced with permission EJCTS 2018 [42] . SVG: saphenous vein graft; Art: arterial grafts; 0 SVG or SVG = 0, total arterial
revascularisation
Count the veins, not the arteries
We know that SVG will develop progressive atherosclerosis and progressively fail in the long term. We
know that, except for a small percentage of arterial grafts failing in the short term due to flow competition
from the native coronary circulation, there is a paucity of evidence to suggest that arterial grafts will ever
progressively fail in the long term. Survival with one or more SVG was lower than for TAR [Figure 6]. The
survival advantage of TAR remained even when there was a majority of grafts that were arterial (multi-
[42]
arterial) and with one SVG [Figure 7].
The relationship between graft failure and reduced survival has a plausible mechanism and therefore it is
suggested that the conduit of most interest is the SVG rather than the arterial conduits [37,38,40,45,46] . It would
be logical, therefore, that the number of SVG grafts has greater effect on survival than the number of
arterial grafts. The strategy of TAR is predicated on the principle of reducing or eliminating SVG grafts,
rather than the principle of greater number of arterial grafts.
Early mortality of TAR
Whilst it is a common belief that TAR is more complex and therefore results in a higher perioperative
mortality, there appears to be very little evidence to support this view. Indeed, the evidence points to a
lower perioperative mortality with TAR [47-49] . There is also a paucity of evidence that “low volume” centres
exhibit a disproportionally higher perioperative mortality with TAR; indeed, the same argument was
present in the 1980s and 1990s when there was resistance to the increased use of IMA [46,50-52] .
Potential risks of multi-arterial grafting
The principle risk of BIMA is a higher rate of deep sternal wound infection. The literature is vast with
considerable debate; however, large-scale or meta-analyses indicate a consistent finding that the rate is
approximately double that of single IMA, higher in diabetics and obese females and possibly lower with
skeletonised IMA [53-56] . Logically, harvesting the IMA by any method substantially reduces the blood supply
to one side of the sternum, and any difference between harvest techniques is not likely to be substantial.
The risks to the forearm following RA harvest are surprisingly low [57-61] . Ischemic complications affecting
the hand are exceptionally rare. Wound infections are infrequent due to the superior blood supply of the
forearm relative to the leg, and nerve damage is confined to local nerves that are entirely cutaneous and
which do not supply the palm or fingertips. There is no evidence that the forearm has reduced blood flow
[62]
following RA harvest .