
Page 122 - Read Online
P. 122
Page 8 of 11 Scirpa et al. Vessel Plus 2022;6:52 https://dx.doi.org/10.20517/2574-1209.2021.74
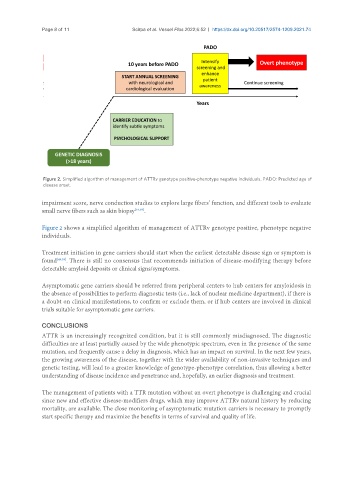
Figure 2. Simplified algorithm of management of ATTRv genotype positive-phenotype negative individuals. PADO: Predicted age of
disease onset.
impairment score, nerve conduction studies to explore large fibers’ function, and different tools to evaluate
small nerve fibers such as skin biopsy [54,58] .
Figure 2 shows a simplified algorithm of management of ATTRv genotype positive, phenotype negative
individuals.
Treatment initiation in gene carriers should start when the earliest detectable disease sign or symptom is
found [49,59] . There is still no consensus that recommends initiation of disease-modifying therapy before
detectable amyloid deposits or clinical signs/symptoms.
Asymptomatic gene carriers should be referred from peripheral centers to hub centers for amyloidosis in
the absence of possibilities to perform diagnostic tests (i.e., lack of nuclear medicine department), if there is
a doubt on clinical manifestations, to confirm or exclude them, or if hub centers are involved in clinical
trials suitable for asymptomatic gene carriers.
CONCLUSIONS
ATTR is an increasingly recognized condition, but it is still commonly misdiagnosed. The diagnostic
difficulties are at least partially caused by the wide phenotypic spectrum, even in the presence of the same
mutation, and frequently cause a delay in diagnosis, which has an impact on survival. In the next few years,
the growing awareness of the disease, together with the wider availability of non-invasive techniques and
genetic testing, will lead to a greater knowledge of genotype-phenotype correlation, thus allowing a better
understanding of disease incidence and penetrance and, hopefully, an earlier diagnosis and treatment.
The management of patients with a TTR mutation without an overt phenotype is challenging and crucial
since new and effective disease-modifiers drugs, which may improve ATTRv natural history by reducing
mortality, are available. The close monitoring of asymptomatic mutation carriers is necessary to promptly
start specific therapy and maximize the benefits in terms of survival and quality of life.