
Page 11 - Read Online
P. 11
Skopis et al. Vessel Plus 2020;4:30 I http://dx.doi.org/10.20517/2574-1209.2020.42 Page 7 of 14
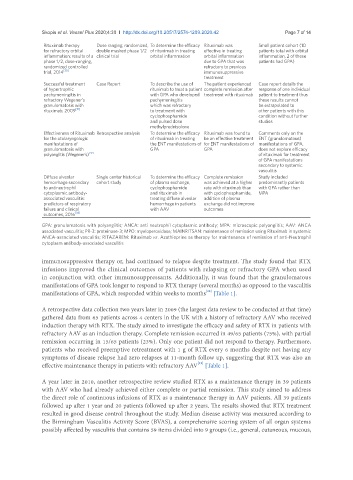
Rituximab therapy Dose ranging, randomized, To determine the efficacy Rituximab was Small patient cohort (10
for refractory orbital double masked phase 1/2 of rituximab in treating effective in treating patients total with orbital
inflammation: results of a clinical trial orbital inflammation orbital inflammation inflammation, 2 of these
phase 1/2, dose-ranging, due to GPA that was patients had GPA)
randomized controlled refractory to previous
trial, 2014 [30] immunosuppressive
treatment
Successful treatment Case Report To describe the use of The patient experienced Case report details the
of hypertrophic rituximab to treat a patient complete remission after response of one individual
pachymeningitis in with GPA who developed treatment with rituximab patient to treatment thus
refractory Wegener’s pachymeningitis these results cannot
granulomatosis with which was refractory be extrapolated to
rituximab, 2009 [31] to treatment with other patients with this
cyclophosphamide condition without further
and pulsed dose studies
methylprednisolone
Effectiveness of Rituximab Retrospective analysis To determine the efficacy Rituximab was found to Comments only on the
for the otolaryngologic of rituximab in treating be an effective treatment ENT (granulomatous)
manifestations of the ENT manifestations of for ENT manifestations of manifestations of GPA,
granulomatosis with GPA GPA does not explore efficacy
polyangiitis (Wegener’s) [32] of rituximab for treatment
of GPA manifestations
secondary to systemic
vasculitis
Diffuse alveolar Single center historical To determine the efficacy Complete remission Study included
hemorrhage secondary cohort study of plasma exchange, was achieved at a higher predominantly patients
to antineutrophil cyclophosphamide rate with rituximab than with GPA rather than
cytoplasmic antibody- and rituximab in with cyclophosphamide, MPA
associated vasculitis: treating diffuse alveolar addition of plasma
predictors of respiratory hemorrhage in patients exchange did not improve
failure and clinical with AAV outcomes
outcomes, 2016 [33]
GPA: granulomatosis with polyangiitis; ANCA: anti neutrophil cytoplasmic antibody; MPA: microscopic polyangiitis; AAV: ANCA
associated vasculitis; PR-3: proteinase-3; MPO: myeloperoxidase; MAINRITSAN: maintenance of remission using Rituximab in systemic
ANCA-associated vasculitis; RITAZAREM: Rituximab vs. Azathioprine as therapy for maintenance of remission of anti-Neutrophil
cytoplasm antibody-associated vasculitis
immunosuppressive therapy or, had continued to relapse despite treatment. The study found that RTX
infusions improved the clinical outcomes of patients with relapsing or refractory GPA when used
in conjunction with other immunosuppressants. Additionally, it was found that the granulomatous
manifestations of GPA took longer to respond to RTX therapy (several months) as opposed to the vasculitis
[18]
manifestations of GPA, which responded within weeks to months [Table 1].
A retrospective data collection two years later in 2009 (the largest data review to be conducted at that time)
gathered data from 65 patients across 4 centers in the UK with a history of refractory AAV who received
induction therapy with RTX. The study aimed to investigate the efficacy and safety of RTX in patients with
refractory AAV as an induction therapy. Complete remission occurred in 49/65 patients (75%), with partial
remission occurring in 15/65 patients (23%). Only one patient did not respond to therapy. Furthermore,
patients who received preemptive retreatment with 1 g of RTX every 6 months despite not having any
symptoms of disease relapse had zero relapses at 11-month follow up, suggesting that RTX was also an
[19]
effective maintenance therapy in patients with refractory AAV [Table 1].
A year later in 2010, another retrospective review studied RTX as a maintenance therapy in 39 patients
with AAV who had already achieved either complete or partial remission. This study aimed to address
the direct role of continuous infusions of RTX as a maintenance therapy in AAV patients. All 39 patients
followed up after 1 year and 20 patients followed up after 2 years. The results showed that RTX treatment
resulted in good disease control throughout the study. Median disease activity was measured according to
the Birmingham Vasculitis Activity Score (BVAS), a comprehensive scoring system of all organ systems
possibly affected by vasculitis that contains 59 items divided into 9 groups (i.e., general, cutaneous, mucous,