
Page 586 - Read Online
P. 586
Page 2 of 15 Lane et al. Plast Aesthet Res 2020;7:51 I http://dx.doi.org/10.20517/2347-9264.2020.106
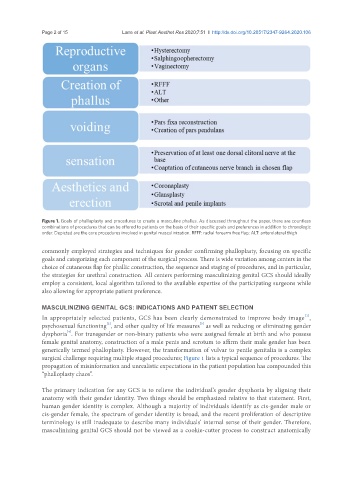
Figure 1. Goals of phalloplasty and procedures to create a masculine phallus. As discussed throughout the paper, there are countless
combinations of procedures that can be offered to patients on the basis of their specific goals and preferences in addition to chronologic
order. Depicted are the core procedures involved in genital masculinization. RFFF: radial forearm free flap; ALT: anterolateral thigh
commonly employed strategies and techniques for gender confirming phalloplasty, focusing on specific
goals and categorizing each component of the surgical process. There is wide variation among centers in the
choice of cutaneous flap for phallic construction, the sequence and staging of procedures, and in particular,
the strategies for urethral construction. All centers performing masculinizing genital GCS should ideally
employ a consistent, local algorithm tailored to the available expertise of the participating surgeons while
also allowing for appropriate patient preference.
MASCULINIZING GENITAL GCS: INDICATIONS AND PATIENT SELECTION
[1]
In appropriately selected patients, GCS has been clearly demonstrated to improve body image ,
[3]
[2]
psychosexual functioning , and other quality of life measures as well as reducing or eliminating gender
[4]
dysphoria . For transgender or non-binary patients who were assigned female at birth and who possess
female genital anatomy, construction of a male penis and scrotum to affirm their male gender has been
generically termed phalloplasty. However, the transformation of vulvar to penile genitalia is a complex
surgical challenge requiring multiple staged procedures; Figure 1 lists a typical sequence of procedures. The
propagation of misinformation and unrealistic expectations in the patient population has compounded this
“phalloplasty chaos”.
The primary indication for any GCS is to relieve the individual’s gender dysphoria by aligning their
anatomy with their gender identity. Two things should be emphasized relative to that statement. First,
human gender identity is complex. Although a majority of individuals identify as cis-gender male or
cis-gender female, the spectrum of gender identity is broad, and the recent proliferation of descriptive
terminology is still inadequate to describe many individuals’ internal sense of their gender. Therefore,
masculinizing genital GCS should not be viewed as a cookie-cutter process to construct anatomically