
Page 123 - Read Online
P. 123
García Botero et al. Plast Aesthet Res 2018;5:15 I http://dx.doi.org/10.20517/2347-9264.2018.09 Page 5 of 8
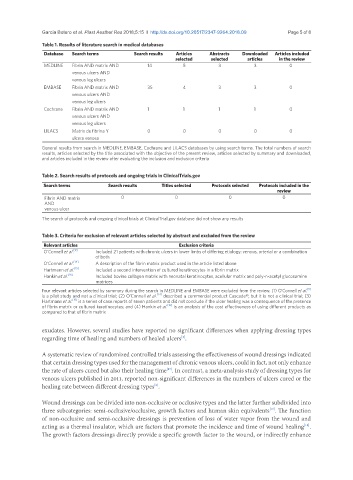
Table 1. Results of literature search in medical databases
Database Search terms Search results Articles Abstracts Downloaded Articles included
selected selected articles in the review
MEDLINE Fibrin AND matrix AND 14 5 3 3 0
venous ulcers AND
venous leg ulcers
EMBASE Fibrin AND matrix AND 35 4 3 3 0
venous ulcers AND
venous leg ulcers
Cochrane Fibrin AND matrix AND 1 1 1 1 0
venous ulcers AND
venous leg ulcers
LILACS Matrix de fibrina Y 0 0 0 0 0
ulcera venosa
General results from search in MEDLINE, EMBASE, Cochrane and LILACS databases by using search terms. The total numbers of search
results, articles selected by the title associated with the objective of the present review, articles selected by summary and downloaded,
and articles included in the review after evaluating the inclusion and exclusion criteria
Table 2. Search results of protocols and ongoing trials in ClinicalTrials.gov
Search terms Search results Titles selected Protocols selected Protocols included in the
review
Fibrin AND matrix 0 0 0 0
AND
venous ulcer
The search of protocols and ongoing clinical trials at ClinicalTrial.gov database did not show any results
Table 3. Criteria for exclusion of relevant articles selected by abstract and excluded from the review
Relevant articles Exclusion criteria
O’Connell et al. [9] Included 21 patients with chronic ulcers in lower limbs of differing etiology: venous, arterial or a combination
of both
O’Connell et al. [14] A description of the fibrin matrix product used in the article listed above
Hartmann et al. [15] Included a second intervention of cultured keratinocytes in a fibrin matrix
Hankin et al. [16] Included bovine collagen matrix with neonatal keratinocytes, acellular matrix and poly-n-acetyl glucosamine
matrices
[9]
Four relevant articles selected by summary during the search in MEDLINE and EMBASE were excluded from the review. (1) O’Connell et al.
is a pilot study and not a clinical trial; (2) O’Connell et al. [14] described a commercial product Cascade®, but it is not a clinical trial; (3)
Hartmann et al. is a series of case reports of seven patients and did not conclude if the ulcer healing was a consequence of the presence
[15]
of fibrin matrix or cultured keratinocytes; and (4) Hankin et al. [16] is an analysis of the cost effectiveness of using different products as
compared to that of fibrin matrix
exudates. However, several studies have reported no significant differences when applying dressing types
regarding time of healing and numbers of healed ulcers .
[2]
A systematic review of randomized controlled trials assessing the effectiveness of wound dressings indicated
that certain dressing types used for the management of chronic venous ulcers, could in fact, not only enhance
the rate of ulcers cured but also their healing time . In contrast, a meta-analysis study of dressing types for
[17]
venous ulcers published in 2011, reported non-significant differences in the numbers of ulcers cured or the
healing rate between different dressing types .
[2]
Wound dressings can be divided into non-occlusive or occlusive types and the latter further subdivided into
three subcategories: semi-occlusive/occlusive, growth factors and human skin equivalents . The function
[17]
of non-occlusive and semi-occlusive dressings is prevention of loss of water vapor from the wound and
acting as a thermal insulator, which are factors that promote the incidence and time of wound healing .
[18]
The growth factors dressings directly provide a specific growth factor to the wound, or indirectly enhance