
Page 81 - Read Online
P. 81
Page 10 of 12 Mitchell et al. Plast Aesthet Res 2023;10:35 https://dx.doi.org/10.20517/2347-9264.2023.14
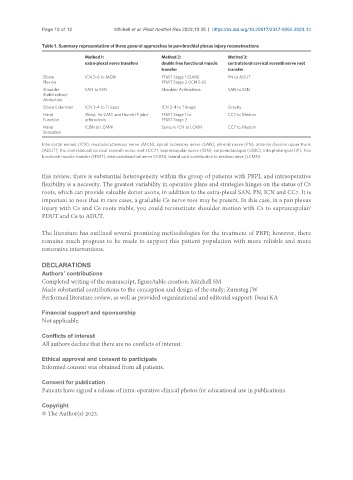
Table 1. Summary representation of three general approaches to pan-brachial plexus injury reconstructions
Method 1: Method 2: Method 3:
extra-plexal nerve transfers double free functional muscle contralateral cervical seventh nerve root
transfer transfer
Elbow ICN 5-6 to MCN FFMT Stage 1 (SAN) PN to ADUT
Flexion FFMT Stage 2 (ICN 5-6)
Shoulder SAN to SSN Shoulder Arthrodesis SAN to SSN
Stabilization/
Abduction
Elbow Extension ICN 3-4 to Triceps ICN 3-4 to Triceps Gravity
Hand Wrist, 1st CMC and thumb IP joint FFMT Stage 1 to CC7 to Median
Function arthrodesis FFMT Stage 2
Hand ICBN to LCMN Sensory ICN to LCMN CC7 to Median
Sensation
Intercostal nerves (ICN), musculocutaneous nerve (MCN), spinal accessory nerve (SAN), phrenic nerve (PN), anterior division upper trunk
(ADUT), the contralateral cervical seventh nerve root (CC7), suprascapular nerve (SSN), carpometacarpal (CMC), interphalangeal (IP), free
functional muscle transfer (FFMT), intercostobrachial nerve (ICBN), lateral cord contribution to median nerve (LCMN)
this review, there is substantial heterogeneity within the group of patients with PBPI, and intraoperative
flexibility is a necessity. The greatest variability in operative plans and strategies hinges on the status of C5
roots, which can provide valuable donor axons, in addition to the extra-plexal SAN, PN, ICN and CC7. It is
important to note that in rare cases, a graftable C6 nerve root may be present. In this case, in a pan plexus
injury with C5 and C6 roots viable, you could reconstitute shoulder motion with C5 to suprascapular/
PDUT and C6 to ADUT.
The literature has outlined several promising methodologies for the treatment of PBPI; however, there
remains much progress to be made to support this patient population with more reliable and more
restorative interventions.
DECLARATIONS
Authors’ contributions
Completed writing of the manuscript, figure/table creation: Mitchell SM
Made substantial contributions to the conception and design of the study: Zumsteg JW
Performed literature review, as well as provided organizational and editorial support: Desai KA
Financial support and sponsorship
Not applicable.
Conflicts of interest
All authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
Informed consent was obtained from all patients.
Consent for publication
Patients have signed a release of intra-operative clinical photos for educational use in publications.
Copyright
© The Author(s) 2023.