
Page 68 - Read Online
P. 68
Page 6 of 10 Schopper et al. Plast Aesthet Res 2022;9:25 https://dx.doi.org/10.20517/2347-9264.2021.72
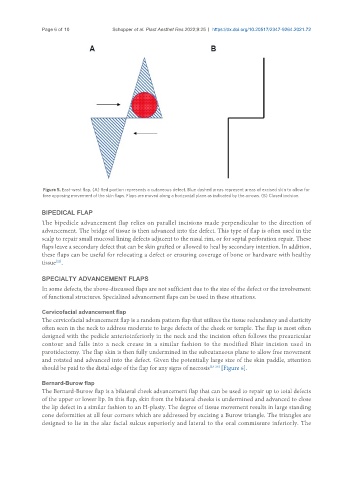
Figure 5. East-west flap. (A) Red portion represents a cutaneous defect. Blue dashed areas represent areas of excised skin to allow for
free opposing movement of the skin flaps. Flaps are moved along a horizontal plane as indicated by the arrows. (B) Closed incision.
BIPEDICAL FLAP
The bipedicle advancement flap relies on parallel incisions made perpendicular to the direction of
advancement. The bridge of tissue is then advanced into the defect. This type of flap is often used in the
scalp to repair small mucosal lining defects adjacent to the nasal rim, or for septal perforation repair. These
flaps leave a secondary defect that can be skin grafted or allowed to heal by secondary intention. In addition,
these flaps can be useful for relocating a defect or ensuring coverage of bone or hardware with healthy
[22]
tissue .
SPECIALTY ADVANCEMENT FLAPS
In some defects, the above-discussed flaps are not sufficient due to the size of the defect or the involvement
of functional structures. Specialized advancement flaps can be used in these situations.
Cervicofacial advancement flap
The cervicofacial advancement flap is a random pattern flap that utilizes the tissue redundancy and elasticity
often seen in the neck to address moderate to large defects of the cheek or temple. The flap is most often
designed with the pedicle anterioinferiorly in the neck and the incision often follows the preauricular
contour and falls into a neck crease in a similar fashion to the modified Blair incision used in
parotidectomy. The flap skin is then fully undermined in the subcutaneous plane to allow free movement
and rotated and advanced into the defect. Given the potentially large size of the skin paddle, attention
should be paid to the distal edge of the flap for any signs of necrosis [23-26] [Figure 6].
Bernard-Burow flap
The Bernard-Burow flap is a bilateral cheek advancement flap that can be used to repair up to total defects
of the upper or lower lip. In this flap, skin from the bilateral cheeks is undermined and advanced to close
the lip defect in a similar fashion to an H-plasty. The degree of tissue movement results in large standing
cone deformities at all four corners which are addressed by excising a Burow triangle. The triangles are
designed to lie in the alar facial sulcus superiorly and lateral to the oral commissure inferiorly. The