
Page 48 - Read Online
P. 48
Page 4 of 8 Rosi-Schumacher et al. Plast Aesthet Res 2022;9:11 https://dx.doi.org/10.20517/2347-9264.2021.64
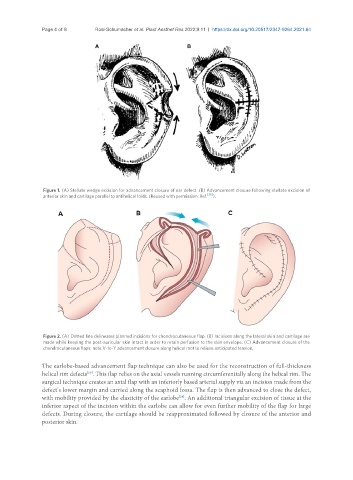
Figure 1. (A) Stellate wedge excision for advancement closure of ear defect. (B) Advancement closure following stellate excision of
anterior skin and cartilage parallel to antihelical folds. (Reused with permission: Ref. [36] ).
Figure 2. (A) Dotted line delineates planned incisions for chondrocutaneous flap. (B) Incisions along the lateral skin and cartilage are
made while keeping the post-auricular skin intact in order to retain perfusion to the skin envelope. (C) Advancement closure of the
chondrocutaneous flaps; note V-to-Y advancement closure along helical root to relieve anticipated tension.
The earlobe-based advancement flap technique can also be used for the reconstruction of full-thickness
[28]
helical rim defects . This flap relies on the axial vessels running circumferentially along the helical rim. The
surgical technique creates an axial flap with an inferiorly based arterial supply via an incision made from the
defect’s lower margin and carried along the scaphoid fossa. The flap is then advanced to close the defect,
with mobility provided by the elasticity of the earlobe . An additional triangular excision of tissue at the
[28]
inferior aspect of the incision within the earlobe can allow for even further mobility of the flap for large
defects. During closure, the cartilage should be reapproximated followed by closure of the anterior and
posterior skin.