
Page 62 - Read Online
P. 62
Seki et al. Plast Aesthet Res 2021;8:44 https://dx.doi.org/10.20517/2347-9264.2021.74 Page 5 of 11
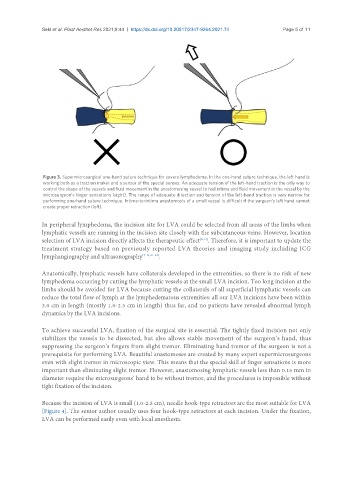
Figure 3. Supermicrosurgical one-hand suture technique for severe lymphedema. In the one-hand suture technique, the left hand is
working both as a traction maker and a sensor of the special senses. An adequate tension of the left-hand traction is the only way to
control the shape of the vessels and fluid movement in the anastomosing vessel to feel intima and fluid movement in the vessel by the
microsurgeon’s finger sensations (right). The range of adequate direction and tension of the left-hand traction is very narrow for
performing one-hand suture technique. Intima-to-intima anastomosis of a small vessel is difficult if the surgeon’s left hand cannot
create proper retraction (left).
In peripheral lymphedema, the incision site for LVA could be selected from all areas of the limbs when
lymphatic vessels are running in the incision site closely with the subcutaneous veins. However, location
selection of LVA incision directly affects the therapeutic effect [8-14] . Therefore, it is important to update the
treatment strategy based on previously reported LVA theories and imaging study including ICG
lymphangiography and ultrasonography [7-14,21-24] .
Anatomically, lymphatic vessels have collaterals developed in the extremities, so there is no risk of new
lymphedema occurring by cutting the lymphatic vessels at the small LVA incision. Too long incision at the
limbs should be avoided for LVA because cutting the collaterals of all superficial lymphatic vessels can
reduce the total flow of lymph at the lymphedematous extremities: all our LVA incisions have been within
3.0 cm in length (mostly 1.0-2.5 cm in length) thus far, and no patients have revealed abnormal lymph
dynamics by the LVA incisions.
To achieve successful LVA, fixation of the surgical site is essential. The tightly fixed incision not only
stabilizes the vessels to be dissected, but also allows stable movement of the surgeon’s hand, thus
suppressing the surgeon’s fingers from slight tremor. Eliminating hand tremor of the surgeon is not a
prerequisite for performing LVA. Beautiful anastomoses are created by many expert supermicrosurgeons
even with slight tremor in microscopic view. This means that the special skill of finger sensations is more
important than eliminating slight tremor. However, anastomosing lymphatic vessels less than 0.15 mm in
diameter require the microsurgeons’ hand to be without tremor, and the procedures is impossible without
tight fixation of the incision.
Because the incision of LVA is small (1.0-2.5 cm), needle hook-type retractors are the most suitable for LVA
[Figure 4]. The senior author usually uses four hook-type retractors at each incision. Under the fixation,
LVA can be performed easily even with local anesthesia.