
Page 112 - Read Online
P. 112
Seki et al. Plast Aesthet Res 2021;8:58 https://dx.doi.org/10.20517/2347-9264.2021.80 Page 5 of 11
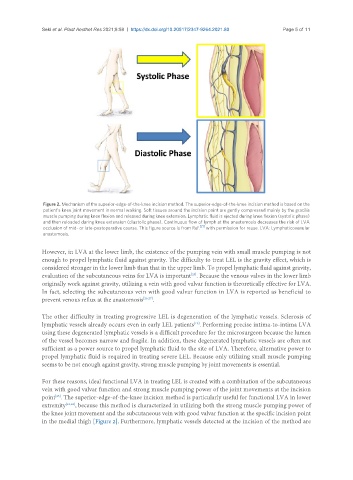
Figure 2. Mechanism of the superior-edge-of-the-knee incision method. The superior-edge-of-the-knee incision method is based on the
patient’s knee joint movement in normal walking. Soft tissues around the incision point are gently compressed mainly by the gracilis
muscle pumping during knee flexion and released during knee extension. Lymphatic fluid is ejected during knee flexion (systolic phase)
and then reloaded during knee extension (diastolic phase). Continuous flow of lymph at the anastomosis decreases the risk of LVA
[21]
occlusion of mid- or late-postoperative course. This figure source is from Ref. with permission for reuse. LVA: Lymphaticovenular
anastomosis.
However, in LVA at the lower limb, the existence of the pumping vein with small muscle pumping is not
enough to propel lymphatic fluid against gravity. The difficulty to treat LEL is the gravity effect, which is
considered stronger in the lower limb than that in the upper limb. To propel lymphatic fluid against gravity,
evaluation of the subcutaneous veins for LVA is important . Because the venous valves in the lower limb
[25]
originally work against gravity, utilizing a vein with good valvar function is theoretically effective for LVA.
In fact, selecting the subcutaneous vein with good valvar function in LVA is reported as beneficial to
prevent venous reflux at the anastomosis [26,27] .
The other difficulty in treating progressive LEL is degeneration of the lymphatic vessels. Sclerosis of
lymphatic vessels already occurs even in early LEL patients . Performing precise intima-to-intima LVA
[19]
using these degenerated lymphatic vessels is a difficult procedure for the microsurgeon because the lumen
of the vessel becomes narrow and fragile. In addition, these degenerated lymphatic vessels are often not
sufficient as a power source to propel lymphatic fluid to the site of LVA. Therefore, alternative power to
propel lymphatic fluid is required in treating severe LEL. Because only utilizing small muscle pumping
seems to be not enough against gravity, strong muscle pumping by joint movements is essential.
For these reasons, ideal functional LVA in treating LEL is created with a combination of the subcutaneous
vein with good valvar function and strong muscle pumping power of the joint movements at the incision
point . The superior-edge-of-the-knee incision method is particularly useful for functional LVA in lower
[25]
extremity [21,22] , because this method is characterized in utilizing both the strong muscle pumping power of
the knee joint movement and the subcutaneous vein with good valvar function at the specific incision point
in the medial thigh [Figure 2]. Furthermore, lymphatic vessels detected at the incision of the method are