
Page 152 - Read Online
P. 152
Nguyen et al. Plast Aesthet Res 2019;6:31 I http://dx.doi.org/10.20517/2347-9264.2019.42 Page 7 of 10
Figure 8. Demonstration of leg extension after free functional gracilis muscle flap to left quadriceps position at three years post-surgery:
(A) leg at rest; (B) full active extension of leg; and (C) skin paddle of flap
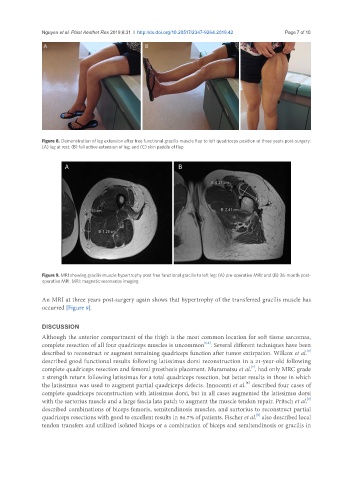
Figure 9. MRI showing gracilis muscle hypertrophy post free functional gracilis to left leg: (A) pre-operative MRI; and (B) 36-month post-
operative MRI. MRI: magnetic resonance imaging
An MRI at three years post-surgery again shows that hypertrophy of the transferred gracilis muscle has
occurred [Figure 9].
DISCUSSION
Although the anterior compartment of the thigh is the most common location for soft tissue sarcomas,
[1,2]
complete resection of all four quadriceps muscles is uncommon . Several different techniques have been
[6]
described to reconstruct or augment remaining quadriceps function after tumor extirpation. Willcox et al.
described good functional results following latissimus dorsi reconstruction in a 21-year-old following
[7]
complete quadriceps resection and femoral prosthesis placement. Muramatsu et al. , had only MRC grade
2 strength return following latissimus for a total quadriceps resection, but better results in those in which
[8]
the latissimus was used to augment partial quadriceps defects. Innocenti et al. described four cases of
complete quadriceps reconstruction with latissimus dorsi, but in all cases augmented the latissimus dorsi
[2]
with the sartorius muscle and a large fascia lata patch to augment the muscle tendon repair. Pritsch et al.
described combinations of biceps femoris, semitendinosis muscles, and sartorius to reconstruct partial
[9]
quadriceps resections with good to excellent results in 86.7% of patients. Fischer et al. also described local
tendon transfers and utilized isolated biceps or a combination of biceps and semitendinosis or gracilis in