
Page 64 - Read Online
P. 64
Page 4 of 15 Tang et al. Plast Aesthet Res 2024;11:61 https://dx.doi.org/10.20517/2347-9264.2024.117
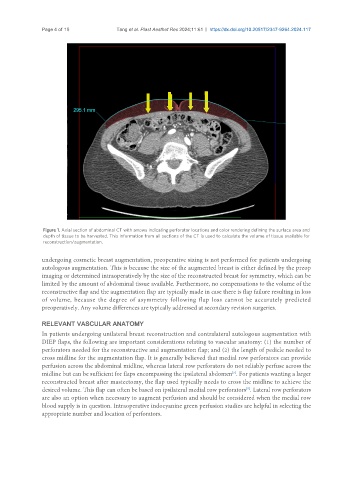
Figure 1. Axial section of abdominal CT with arrows indicating perforator locations and color rendering defining the surface area and
depth of tissue to be harvested. This information from all sections of the CT is used to calculate the volume of tissue available for
reconstruction/augmentation.
undergoing cosmetic breast augmentation, preoperative sizing is not performed for patients undergoing
autologous augmentation. This is because the size of the augmented breast is either defined by the preop
imaging or determined intraoperatively by the size of the reconstructed breast for symmetry, which can be
limited by the amount of abdominal tissue available. Furthermore, no compensations to the volume of the
reconstructive flap and the augmentation flap are typically made in case there is flap failure resulting in loss
of volume, because the degree of asymmetry following flap loss cannot be accurately predicted
preoperatively. Any volume differences are typically addressed at secondary revision surgeries.
RELEVANT VASCULAR ANATOMY
In patients undergoing unilateral breast reconstruction and contralateral autologous augmentation with
DIEP flaps, the following are important considerations relating to vascular anatomy: (1) the number of
perforators needed for the reconstructive and augmentation flap; and (2) the length of pedicle needed to
cross midline for the augmentation flap. It is generally believed that medial row perforators can provide
perfusion across the abdominal midline, whereas lateral row perforators do not reliably perfuse across the
midline but can be sufficient for flaps encompassing the ipsilateral abdomen . For patients wanting a larger
[5]
reconstructed breast after mastectomy, the flap used typically needs to cross the midline to achieve the
desired volume. This flap can often be based on ipsilateral medial row perforators . Lateral row perforators
[5]
are also an option when necessary to augment perfusion and should be considered when the medial row
blood supply is in question. Intraoperative indocyanine green perfusion studies are helpful in selecting the
appropriate number and location of perforators.