
Page 538 - Read Online
P. 538
Page 8 of 15 Pusca et al. Mini-invasive Surg 2021;5:51 https://dx.doi.org/10.20517/2574-1225.2021.45
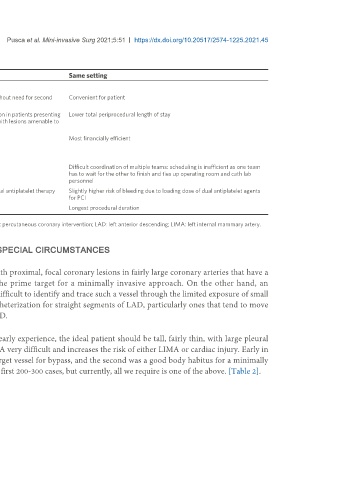
Table 1. Comparison of the three strategies available to perform the steps of HCR
Minimally invasive CABG first Stent first Same setting
Advantages
Less risk of bleeding during the CABG Bails out to conventional surgery if PCI unsuccessful without need for second Convenient for patient
surgery; helpful option for CTO PCI of non-LAD vessels
LIMA LAD provides protection during Allows immediate, expeditious coronary revascularization in patients presenting Lower total periprocedural length of stay
subsequent PCI with acute coronary syndromes in non-LAD territories with lesions amenable to
PCI
Able to study the LIMA LAD anastomosis at time Most financially efficient
of subsequent PCI
Disadvantages
Incomplete revascularization during the higher No LIMA LAD protection for multivessel PCI Difficult coordination of multiple teams: scheduling is inefficient as one team
cardiac demands of postoperative recovery has to wait for the other to finish and ties up operating room and cath lab
personnel
Unsuccessful PCI requires a second surgery Highest risk of bleeding during CABG due to need for dual antiplatelet therapy Slightly higher risk of bleeding due to loading dose of dual antiplatelet agents
after stent (extended administration) for PCI
Requires two separate procedures Requires two separate procedures Longest procedural duration
HCR: Hybrid coronary revascularization; CABG: coronary artery bypass; CTO: complete total occlusion; PCI: percutaneous coronary intervention; LAD: left anterior descending; LIMA: left internal mammary artery.
SELECTION OF PATIENTS FOR HCR AND PERFORMING HCR IN SPECIAL CIRCUMSTANCES
The ideal candidate for HCR
Experience has taught us that the best-suited patients for HCR are the ones with proximal, focal coronary lesions in fairly large coronary arteries that have a
relatively low burden of calcium. Thus, the mid or mid to distal LAD is the prime target for a minimally invasive approach. On the other hand, an
intramyocardial LAD is a relative contraindication for HCR because it is very difficult to identify and trace such a vessel through the limited exposure of small
thoracotomy attention should be paid to examine the preoperative cardiac catheterization for straight segments of LAD, particularly ones that tend to move
inward in systole more than the rest of the LAD, and particularly in the mid LAD.
Body habitus plays a significant role in the success of HCR. In the surgeon’s early experience, the ideal patient should be tall, fairly thin, with large pleural
cavities and a relatively small heart. A large heart can make harvesting the LIMA very difficult and increases the risk of either LIMA or cardiac injury. Early in
our experience, we required two criteria for inclusion: one was a good LAD target vessel for bypass, and the second was a good body habitus for a minimally
invasive left thoracotomy approach. We adhered strictly to this protocol for the first 200-300 cases, but currently, all we require is one of the above. [Table 2].