
Page 28 - Read Online
P. 28
Ugliono et al. Mini-invasive Surg 2021;5:2 I http://dx.doi.org/10.20517/2574-1225.2020.93 Page 5 of 12
Figure 3. Identification of the hernia sac
A B
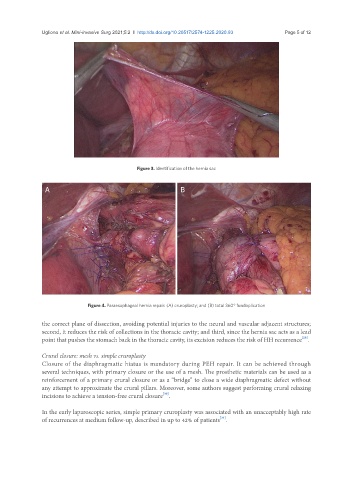
Figure 4. Paraesophageal hernia repair: (A) cruroplasty; and (B) total 360° fundoplication
the correct plane of dissection, avoiding potential injuries to the neural and vascular adjacent structures;
second, it reduces the risk of collections in the thoracic cavity; and third, since the hernia sac acts as a lead
point that pushes the stomach back in the thoracic cavity, its excision reduces the risk of HH recurrence .
[29]
Crural closure: mesh vs. simple cruroplasty
Closure of the diaphragmatic hiatus is mandatory during PEH repair. It can be achieved through
several techniques, with primary closure or the use of a mesh. The prosthetic materials can be used as a
reinforcement of a primary crural closure or as a “bridge” to close a wide diaphragmatic defect without
any attempt to approximate the crural pillars. Moreover, some authors suggest performing crural relaxing
[30]
incisions to achieve a tension-free crural closure .
In the early laparoscopic series, simple primary cruroplasty was associated with an unacceptably high rate
of recurrences at medium follow-up, described in up to 42% of patients .
[31]