
Page 749 - Read Online
P. 749
Page 18 of 24 Palacios Mini-invasive Surg 2020;4:73 I http://dx.doi.org/10.20517/2574-1225.2020.72
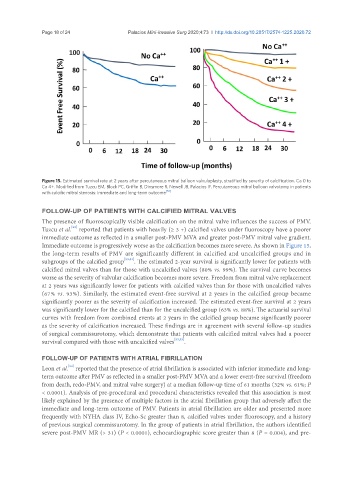
Figure 15. Estimated survival rate at 2 years after percutaneous mitral balloon valvuloplasty, stratified by severity of calcification. Ca 0 to
Ca 4+. Modified from Tuzcu EM, Block PC, Griffin B, Dinsmore R, Newell JB, Palacios IF. Percutaneous mitral balloon valvotomy in patients
with calcific mitral stenosis: immediate and long-term outcome [53]
FOLLOW-UP OF PATIENTS WITH CALCIFIED MITRAL VALVES
The presence of fluoroscopically visible calcification on the mitral valve influences the success of PMV.
[53]
Tuzcu et al. reported that patients with heavily (≥ 3 +) calcified valves under fluoroscopy have a poorer
immediate outcome as reflected in a smaller post-PMV MVA and greater post-PMV mitral valve gradient.
Immediate outcome is progressively worse as the calcification becomes more severe. As shown in Figure 15,
the long-term results of PMV are significantly different in calcified and uncalcified groups and in
subgroups of the calcified group [53,54] . The estimated 2-year survival is significantly lower for patients with
calcified mitral valves than for those with uncalcified valves (80% vs. 99%). The survival curve becomes
worse as the severity of valvular calcification becomes more severe. Freedom from mitral valve replacement
at 2 years was significantly lower for patients with calcified valves than for those with uncalcified valves
(67% vs. 93%). Similarly, the estimated event-free survival at 2 years in the calcified group became
significantly poorer as the severity of calcification increased. The estimated event-free survival at 2 years
was significantly lower for the calcified than for the uncalcified group (63% vs. 88%). The actuarial survival
curves with freedom from combined events at 2 years in the calcified group became significantly poorer
as the severity of calcification increased. These findings are in agreement with several follow-up studies
of surgical commissurotomy, which demonstrate that patients with calcified mitral valves had a poorer
survival compared with those with uncalcified valves [53,55] .
FOLLOW-UP OF PATIENTS WITH ATRIAL FIBRILLATION
[54]
Leon et al. reported that the presence of atrial fibrillation is associated with inferior immediate and long-
term outcome after PMV as reflected in a smaller post-PMV MVA and a lower event-free survival (freedom
from death, redo-PMV, and mitral valve surgery) at a median follow-up time of 61 months (32% vs. 61%; P
< 0.0001). Analysis of pre-procedural and procedural characteristics revealed that this association is most
likely explained by the presence of multiple factors in the atrial fibrillation group that adversely affect the
immediate and long-term outcome of PMV. Patients in atrial fibrillation are older and presented more
frequently with NYHA class IV, Echo-Sc greater than 8, calcified valves under fluoroscopy, and a history
of previous surgical commissurotomy. In the group of patients in atrial fibrillation, the authors identified
severe post-PMV MR (> 31) (P < 0.0001), echocardiographic score greater than 8 (P = 0.004), and pre-