
Page 63 - Read Online
P. 63
Yuu et al. Mini-invasive Surg 2019;3:6 I http://dx.doi.org/10.20517/2574-1225.2018.73 Page 5 of 9
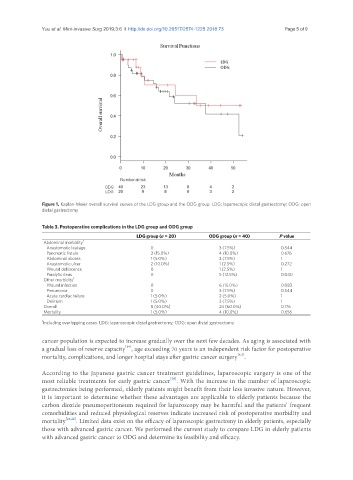
Figure 1. Kaplan-Meier overall survival curves of the LDG group and the ODG group. LDG: laparoscopic distal gastrectomy; ODG: open
distal gastrectomy
Table 3. Postoperative complications in the LDG group and ODG group
LDG group (n = 20) ODG group (n = 40) P value
Abdominal morbidity 1
Anastomotic leakage 0 3 (7.5%) 0.544
Pancreatic fistula 3 (15.0%) 4 (10.0%) 0.676
Abdominal abcess 1 (5.0%) 3 (7.5%) 1
Anastomotic ulcer 2 (10.0%) 1 (2.5%) 0.272
Wound dehiscence 0 1 (2.5%) 1
Paralytic ileus 0 5 (12.5%) 0.040
Other morbidity 1
Wound infection 0 6 (15.0%) 0.083
Pneumonia 0 3 (7.5%) 0.544
Acute cardiac failure 1 (5.0%) 2 (5.0%) 1
Delirium 1 (5.0%) 3 (7.5%) 1
Overall 8 (40.0%) 24 (60.0%) 0.176
Mortality 1 (5.0%) 4 (10.0%) 0.656
1 Including overlapping cases. LDG: laparoscopic distal gastrectomy; ODG: open distal gastrectomy
cancer population is expected to increase gradually over the next few decades. As aging is associated with
[19]
a gradual loss of reserve capacity , age exceeding 70 years is an independent risk factor for postoperative
[4,5]
mortality, complications, and longer hospital stays after gastric cancer surgery .
According to the Japanese gastric cancer treatment guidelines, laparoscopic surgery is one of the
[20]
most reliable treatments for early gastric cancer . With the increase in the number of laparoscopic
gastrectomies being performed, elderly patients might benefit from their less invasive nature. However,
it is important to determine whether these advantages are applicable to elderly patients because the
carbon dioxide pneumoperitoneum required for laparoscopy may be harmful and the patients’ frequent
comorbidities and reduced physiological reserves indicate increased risk of postoperative morbidity and
mortality [21,22] . Limited data exist on the efficacy of laparoscopic gastrectomy in elderly patients, especially
those with advanced gastric cancer. We performed the current study to compare LDG in elderly patients
with advanced gastric cancer to ODG and determine its feasibility and efficacy.