
Page 162 - Read Online
P. 162
Page 6 of 14 Parthasarathi et al. Mini-invasive Surg 2019;3:20 I http://dx.doi.org/10.20517/2574-1225.2019.10
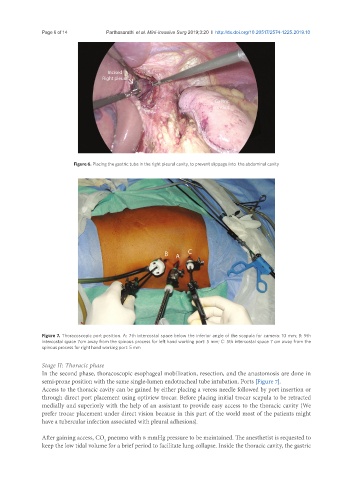
Figure 6. Placing the gastric tube in the right pleural cavity, to prevent slippage into the abdominal cavity
Figure 7. Thoracoscopic port position. A: 7th intercostal space below the inferior angle of the scapula for camera: 10 mm; B: 9th
intercostal space 7cm away from the spinous process for left hand working port: 5 mm; C: 5th intercostal space 7 cm away from the
spinous process for right hand working port: 5 mm
Stage II: Thoracic phase
In the second phase, thoracoscopic esophageal mobilization, resection, and the anastomosis are done in
semi-prone position with the same single-lumen endotracheal tube intubation. Ports [Figure 7].
Access to the thoracic cavity can be gained by either placing a veress needle followed by port insertion or
through direct port placement using optiview trocar. Before placing initial trocar scapula to be retracted
medially and superiorly with the help of an assistant to provide easy access to the thoracic cavity (We
prefer trocar placement under direct vision because in this part of the world most of the patients might
have a tubercular infection associated with pleural adhesions).
After gaining access, CO pneumo with 8 mmHg pressure to be maintained. The anesthetist is requested to
2
keep the low tidal volume for a brief period to facilitate lung collapse. Inside the thoracic cavity, the gastric