
Page 50 - Read Online
P. 50
Page 4 of 9 Yoshizaki et al. Mini-invasive Surg 2022;6:17 https://dx.doi.org/10.20517/2574-1225.2021.116
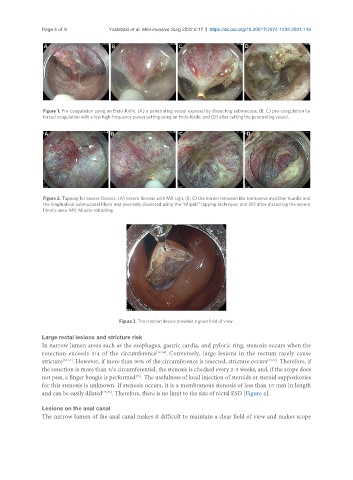
Figure 1. Pre-coagulation using an Endo-Knife: (A) a penetrating vessel exposed by dissecting submucosa; (B, C) pre-coagulation by
forced coagulation with a low high-frequency power setting using an Endo-Knife; and (D) after cutting the penetrating vessel.
Figure 2. Tapping for severe fibrosis: (A) severe fibrosis with MR sign; (B, C) the border between the transverse myofiber bundle and
the longitudinal submucosal fibers was precisely dissected using the “Migaki” tapping technique; and (D) after dissecting the severe
fibrotic area. MR: Muscle retracting.
Figure 3. The traction device provides a good field of view.
Large rectal lesions and stricture risk
In narrow lumen areas such as the esophagus, gastric cardia, and pyloric ring, stenosis occurs when the
resection exceeds 3/4 of the circumference [32-34] . Conversely, large lesions in the rectum rarely cause
stricture [35-37] . However, if more than 90% of the circumference is resected, stricture occurs [35,36] . Therefore, if
the resection is more than 3/4 circumferential, the stenosis is checked every 2-3 weeks, and, if the scope does
not pass, a finger bougie is performed . The usefulness of local injection of steroids or steroid suppositories
[35]
for this stenosis is unknown. If stenosis occurs, it is a membranous stenosis of less than 10 mm in length
and can be easily dilated [35,36] . Therefore, there is no limit to the size of rectal ESD [Figure 4].
Lesions on the anal canal
The narrow lumen of the anal canal makes it difficult to maintain a clear field of view and makes scope