
Page 81 - Read Online
P. 81
Maqboul et al. Mini-invasive Surg 2021;5:44 https://dx.doi.org/10.20517/2574-1225.2021.54 Page 15 of 19
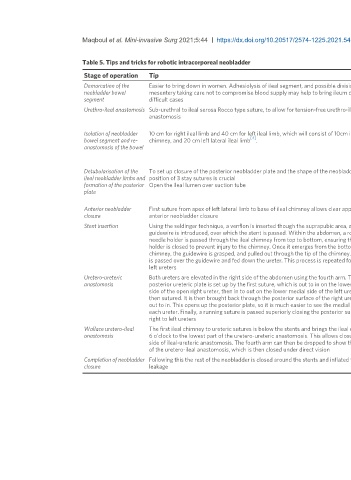
Table 5. Tips and tricks for robotic intracorporeal neobladder
Stage of operation Tip Challenge and possible complication Figure
Demarcation of the Easier to bring down in women. Adhesiolysis of ileal segment, and possible division of Inability to bring the ileum into the pelvis may result in conversion to Figure 1
neobladder bowel mesentery taking care not to compromise blood supply may help to bring ileum down in ileal conduit
segment difficult cases
Urethro-ileal anastomosis Sub-urethral to ileal serosa Rocco type suture, to allow for tension-free urethro-ileal Without being tension-free, the anastomosis may break down, Figures 2 and 3
anastomosis notwithstanding technical difficulty of suturing without losing its
stabilizing effect
Isolation of neobladder 10 cm for right ileal limb and 40 cm for left ileal limb, which will consist of 10cm ileal Position of bowel that is re-anastomosed within right side of abdomen, Figure 4
[4]
bowel segment and re- chimney, and 20 cm left lateral ileal limb . and angle of stapler determined by fourth arm trocar position is
anastomosis of the bowel important. Re-anastomosis is done by using 60 mm then 45 mm staples,
then closed with final 60 mm staples. Anastomotic leak is a potential
complication
Detubularisation of the To set up closure of the posterior neobladder plate and the shape of the neobladder the Opening ileal lumen over the suction tube helps prevent injury to Figures 5 and 6
ileal neobladder limbs and position of 3 stay sutures is crucial posterior wall of the ileum. Judicious placement of 3 stay sutures limits
formation of the posterior Open the ileal lumen over suction tube technical difficulty of suturing posterior plate of the neobladder and
plate eases later folding and anterior closure. Potential complications include
injury to posterior ileal wall and posterior neobladder leak or rupture
Anterior neobladder First suture from apex of left lateral limb to base of ileal chimney allows clear approach for Judicious suturing will prevent neobladder leak or rupture Figures 7-9
closure anterior neobladder closure
Stent insertion Using the seldinger technique, a venflon is inserted though the suprapubic area, and a The robotic needle holder has to pass down the ileal chimney carefully to Figure 10
guidewire is introduced, over which the stent is passed. Within the abdomen, a robotic prevent injury, and later the stents must be pushed into the renal
needle holder is passed through the ileal chimney from top to bottom, ensuring the needle collecting system. They are sutured together to the skin of the anterior
holder is closed to prevent injury to the chimney. Once it emerges from the bottom of the abdominal wall and removed at 14 days. They allow the uretero-ureteric
chimney, the guidewire is grasped, and pulled out through the tip of the chimney. The stent and uretero-ileal anastomoses to heal, and help to prevent ureteric
is passed over the guidewire and fed down the ureter. This process is repeated for right and stricturing, anastomotic breakdown and leakage
left ureters
Uretero-ureteric Both ureters are elevated in the right side of the abdomen using the fourth arm. The The orientation of the suturing should be followed meticulously to allow Figures 11-14
anastomosis posterior ureteric plate is set up by the first suture, which is out to in on the lower medial efficient progress. Poor technique may cause anastomotic leakage and
side of the open right ureter, then in to out on the lower medial side of the left ureter, and ureteric strictures
then sutured. It is then brought back through the posterior surface of the right ureter from
out to in. This opens up the posterior plate, so it is much easier to see the medial edges of
each ureter. Finally, a running suture is passed superiorly closing the posterior surface of
right to left ureters
Wallace uretero-ileal The first ileal chimney to ureteric sutures is below the stents and brings the ileal chimney at One of the most technically challenging parts of the procedures, and Figures 15-17
anastomosis 6 o’clock to the lowest part of the uretero-ureteric anastomosis. This allows closure of right important at the beginning to keep sutures below the stents. Poor
side of ileal-ureteric anastomosis. The fourth arm can then be dropped to show the left side technique may cause anastomotic breakdown and leakage
of the uretero-ileal anastomosis, which is then closed under direct vision
Completion of neobladder Following this the rest of the neobladder is closed around the stents and inflated to test for Judicious suturing to ensure tight closure. Potential complication is Figure 18
closure leakage neobladder leak