
Page 62 - Read Online
P. 62
Gharagozloo et al. Mini-invasive Surg 2020;4:66 I http://dx.doi.org/10.20517/2574-1225.2020.53 Page 3 of 22
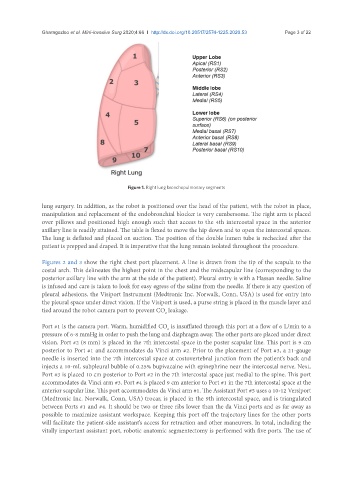
Figure 1. Right lung bronchopulmonary segments
lung surgery. In addition, as the robot is positioned over the head of the patient, with the robot in place,
manipulation and replacement of the endobronchial blocker is very cumbersome. The right arm is placed
over pillows and positioned high enough such that access to the 4th intercostal space in the anterior
axillary line is readily attained. The table is flexed to move the hip down and to open the intercostal spaces.
The lung is deflated and placed on suction. The position of the double lumen tube is rechecked after the
patient is prepped and draped. It is imperative that the lung remain isolated throughout the procedure.
Figures 2 and 3 show the right chest port placement. A line is drawn from the tip of the scapula to the
costal arch. This delineates the highest point in the chest and the midscapular line (corresponding to the
posterior axillary line with the arm at the side of the patient). Pleural entry is with a Hassan needle. Saline
is infused and care is taken to look for easy egress of the saline from the needle. If there is any question of
pleural adhesions, the Visiport Instrument (Medtronic Inc. Norwalk, Conn, USA) is used for entry into
the pleural space under direct vision. If the Visiport is used, a purse string is placed in the muscle layer and
tied around the robot camera port to prevent CO leakage.
2
Port #1 is the camera port. Warm, humidified CO is insufflated through this port at a flow of 6 L/min to a
2
pressure of 6-8 mmHg in order to push the lung and diaphragm away. The other ports are placed under direct
vision. Port #2 (8 mm) is placed in the 7th intercostal space in the poster scapular line. This port is 9 cm
posterior to Port #1 and accommodates da Vinci arm #2. Prior to the placement of Port #3, a 21-gauge
needle is inserted into the 7th intercostal space at costovertebral junction from the patient’s back and
injects a 10-mL subpleural bubble of 0.25% bupivacaine with epinephrine near the intercostal nerve. Next,
Port #3 is placed 10 cm posterior to Port #2 in the 7th intercostal space just medial to the spine. This port
accommodates da Vinci arm #3. Port #4 is placed 9 cm anterior to Port #1 in the 7th intercostal space at the
anterior scapular line. This port accommodates da Vinci arm #1. The Assistant Port #5 uses a 10-12 Versiport
(Medtronic Inc. Norwalk, Conn, USA) trocar, is placed in the 9th intercostal space, and is triangulated
between Ports #1 and #4. It should be two or three ribs lower than the da Vinci ports and as far away as
possible to maximize assistant workspace. Keeping this port off the trajectory lines for the other ports
will facilitate the patient-side assistant’s access for retraction and other maneuvers. In total, including the
vitally important assistant port, robotic anatomic segmentectomy is performed with five ports. The use of