
Page 21 - Read Online
P. 21
Brandolini. Mini-invasive Surg 2020;4:45 I http://dx.doi.org/10.20517/2574-1225.2020.27 Page 7 of 9
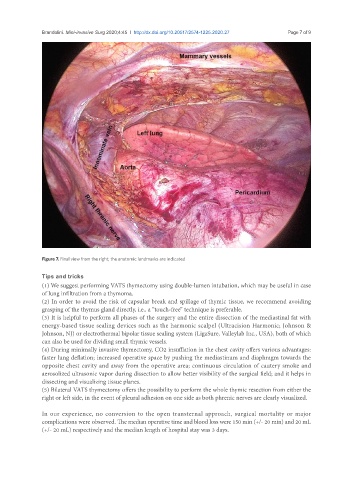
Figure 7. Final view from the right; the anatomic landmarks are indicated
Tips and tricks
(1) We suggest performing VATS thymectomy using double-lumen intubation, which may be useful in case
of lung infiltration from a thymoma.
(2) In order to avoid the risk of capsular break and spillage of thymic tissue, we recommend avoiding
grasping of the thymus gland directly, i.e., a “touch-free” technique is preferable.
(3) It is helpful to perform all phases of the surgery and the entire dissection of the mediastinal fat with
energy-based tissue sealing devices such as the harmonic scalpel (Ultracision Harmonic; Johnson &
Johnson, NJ) or electrothermal bipolar tissue sealing system (LigaSure, Valleylab Inc., USA), both of which
can also be used for dividing small thymic vessels.
(4) During minimally invasive thymectomy, CO2 insufflation in the chest cavity offers various advantages:
faster lung deflation; increased operative space by pushing the mediastinum and diaphragm towards the
opposite chest cavity and away from the operative area; continuous circulation of cautery smoke and
aerosolized ultrasonic vapor during dissection to allow better visibility of the surgical field; and it helps in
dissecting and visualizing tissue planes.
(5) Bilateral VATS thymectomy offers the possibility to perform the whole thymic resection from either the
right or left side, in the event of pleural adhesion on one side as both phrenic nerves are clearly visualized.
In our experience, no conversion to the open transternal approach, surgical mortality or major
complications were observed. The median operative time and blood loss were 150 min (+/- 20 min) and 20 mL
(+/- 20 mL) respectively and the median length of hospital stay was 3 days.