
Page 57 - Read Online
P. 57
Belli et al. Mini-invasive Surg 2020;4:77 I http://dx.doi.org/10.20517/2574-1225.2020.70 Page 5 of 12
§
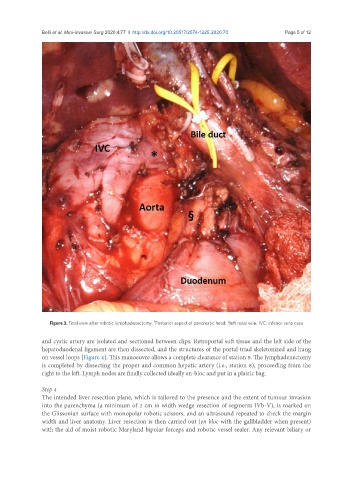
Figure 3. Final view after robotic lymphadenectomy. Posterior aspect of pancreatic head; *left renal vein. IVC: inferior vena cava
and cystic artery are isolated and sectioned between clips. Retroportal soft tissue and the left side of the
hepatoduodenal ligament are then dissected, and the structures of the portal triad skeletonized and hung
on vessel loops [Figure 4]. This manoeuvre allows a complete clearance of station 9. The lymphadenectomy
is completed by dissecting the proper and common hepatic artery (i.e., station 8), proceeding from the
right to the left. Lymph nodes are finally collected ideally en-bloc and put in a plastic bag.
Step 4
The intended liver resection plane, which is tailored to the presence and the extent of tumour invasion
into the parenchyma (a minimum of 2 cm in width wedge resection of segments IVb-V), is marked on
the Glissonian surface with monopolar robotic scissors, and an ultrasound repeated to check the margin
width and liver anatomy. Liver resection is then carried out (en bloc with the gallbladder when present)
with the aid of moist robotic Maryland bipolar forceps and robotic vessel sealer. Any relevant biliary or