
Page 12 - Read Online
P. 12
Page 450 Aledo-Serrano et al. J Transl Genet Genom 2021;5:443-55 https://dx.doi.org/10.20517/jtgg.2021.40
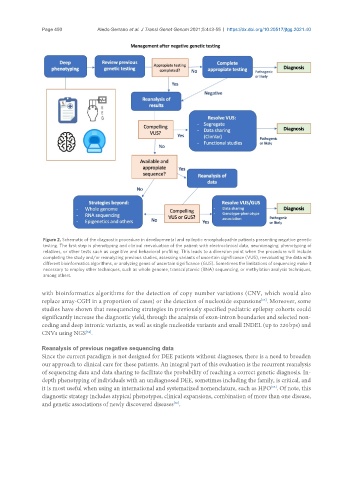
Figure 2. Schematic of the diagnostic procedure in developmental and epileptic encephalopathie patients presenting negative genetic
testing. The first step is phenotyping and clinical reevaluation of the patient with electroclinical data, neuroimaging, phenotyping of
relatives, or other tests such as cognitive and behavioral profiling. This leads to a diversion point when the procedure will include
completing the study and/or reanalyzing previous studies, assessing variants of uncertain significance (VUS), reevaluating the data with
different bioinformatics algorithms, or analyzing genes of uncertain significance (GUS). Sometimes the limitations of sequencing make it
necessary to employ other techniques, such as whole genome, transcriptomic (RNA) sequencing, or methylation analysis techniques,
among others.
with bioinformatics algorithms for the detection of copy number variations (CNV, which would also
replace array-CGH in a proportion of cases) or the detection of nucleotide expansions . Moreover, some
[63]
studies have shown that resequencing strategies in previously specified pediatric epilepsy cohorts could
significantly increase the diagnostic yield, through the analysis of exon-intron boundaries and selected non-
coding and deep intronic variants, as well as single nucleotide variants and small INDEL (up to 220 bps) and
CNVs using NGS .
[64]
Reanalysis of previous negative sequencing data
Since the current paradigm is not designed for DEE patients without diagnoses, there is a need to broaden
our approach to clinical care for these patients. An integral part of this evaluation is the recurrent reanalysis
of sequencing data and data sharing to facilitate the probability of reaching a correct genetic diagnosis. In-
depth phenotyping of individuals with an undiagnosed DEE, sometimes including the family, is critical, and
[65]
it is most useful when using an international and systematized nomenclature, such as HPO . Of note, this
diagnostic strategy includes atypical phenotypes, clinical expansions, combination of more than one disease,
and genetic associations of newly discovered diseases .
[66]