
Page 61 - Read Online
P. 61
Ciolino et al. J Transl Genet Genom 2022;6:429-42 https://dx.doi.org/10.20517/jtgg.2022.15 Page 437
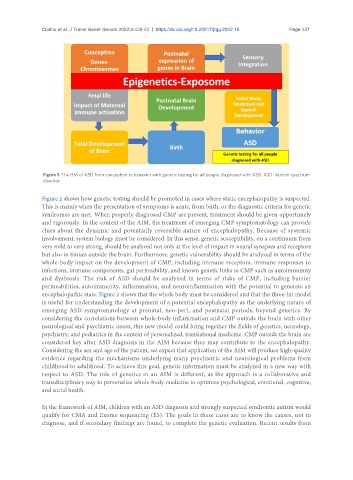
Figure 1. The GM of ASD from conception to behavior with genetic testing for all people diagnosed with ASD. ASD: Autism spectrum
disorder.
Figure 2 shows how genetic testing should be promoted in cases where static encephalopathy is suspected.
This is mainly when the presentation of symptoms is acute, from birth, or the diagnostic criteria for genetic
syndromes are met. When properly diagnosed CMP are present, treatment should be given opportunely
and rigorously. In the context of the AIM, the treatment of emerging CMP symptomatology can provide
clues about the dynamic and potentially reversible nature of encephalopathy. Because of systemic
involvement, system biology must be considered. In this sense, genetic susceptibility, on a continuum from
very mild to very strong, should be analyzed not only at the level of impact in neural synapses and receptors
but also in tissues outside the brain. Furthermore, genetic vulnerability should be analyzed in terms of the
whole-body impact on the development of CMP, including immune receptors, immune responses to
infections, immune components, gut permeability, and known genetic links to CMP such as autoimmunity
and dysbiosis. The risk of ASD should be analyzed in terms of risks of CMP, including barrier
permeabilities, autoimmunity, inflammation, and neuroinflammation with the potential to generate an
encephalopathic state. Figure 2 shows that the whole body must be considered and that the three-hit model
is useful for understanding the development of a potential encephalopathy as the underlying nature of
emerging ASD symptomatology at prenatal, neo-peri, and postnatal periods, beyond genetics. By
considering the correlations between whole-body inflammation and CMP outside the brain with other
neurological and psychiatric issues, this new model could bring together the fields of genetics, neurology,
psychiatry, and pediatrics in the context of personalized, translational medicine. CMP outside the brain are
considered key after ASD diagnosis in the AIM because they may contribute to the encephalopathy.
Considering the sex and age of the patient, we expect that application of the AIM will produce high-quality
evidence regarding the mechanisms underlying many psychiatric and neurological problems from
childhood to adulthood. To achieve this goal, genetic information must be analyzed in a new way with
respect to ASD. The role of genetics in an AIM is different, as the approach is a collaborative and
transdisciplinary way to personalize whole-body medicine to optimize psychological, emotional, cognitive,
and social health.
In the framework of AIM, children with an ASD diagnosis and strongly suspected syndromic autism would
qualify for CMA and Exome sequencing (ES). The goals in these cases are to know the causes, not to
diagnose, and if secondary findings are found, to complete the genetic evaluation. Recent results from