
Page 68 - Read Online
P. 68
Marquina et al. J Cancer Metastasis Treat 2020;6:6 I http://dx.doi.org/10.20517/2394-4722.2019.39 Page 5 of 8
Table 5. The 24- and 48-h goals for correction of chronic hyponatremia (adapted from [22] )
Minimum 24 h SNa Maximum 24 h SNa Maximum 48 h SNa
ODS risk 24 h Goal (mmol/L) 48 h Goal (mmol/L)
rise (mmol/L) rise (mmol/L) rise (mmol/L)
Low 4-8 6-8 10-12 6-8 18
High 4-6 6 8 4-6 8/day
ODS: osmotic demyelination syndrome; SNa: serum sodium
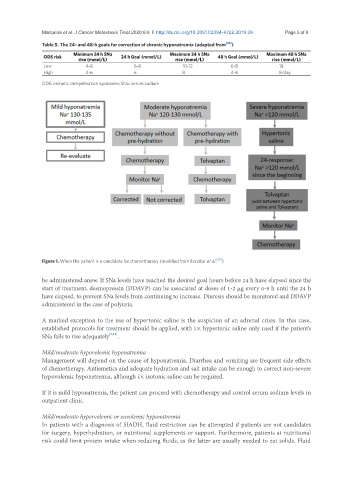
Figure 1. When the patient is a candidate for chemotherapy (modified from Escobar et al. [29] )
be administered anew. If SNa levels have reached the desired goal hours before 24 h have elapsed since the
start of treatment, desmopressin (DDAVP) can be associated at doses of 1-2 μg every 6-8 h until the 24 h
have elapsed, to prevent SNa levels from continuing to increase. Diuresis should be monitored and DDAVP
administered in the case of polyuria.
A marked exception to the use of hypertonic saline is the suspicion of an adrenal crisis. In this case,
established protocols for treatment should be applied, with i.v. hypertonic saline only used if the patient’s
SNa fails to rise adequately [2,19] .
Mild/moderate hypovolemic hyponatremia
Management will depend on the cause of hyponatremia. Diarrhea and vomiting are frequent side effects
of chemotherapy. Antiemetics and adequate hydration and salt intake can be enough to correct non-severe
hypovolemic hyponatremia, although i.v. isotonic saline can be required.
If it is mild hyponatremia, the patient can proceed with chemotherapy and control serum sodium levels in
outpatient clinic.
Mild/moderate hypervolemic or euvolemic hyponatremia
In patients with a diagnosis of SIADH, fluid restriction can be attempted if patients are not candidates
for surgery, hyperhydration, or nutritional supplements or support. Furthermore, patients at nutritional
risk could limit protein intake when reducing fluids, as the latter are usually needed to eat solids. Fluid