
Page 67 - Read Online
P. 67
Page 4 of 8 Marquina et al. J Cancer Metastasis Treat 2020;6:6 I http://dx.doi.org/10.20517/2394-4722.2019.39
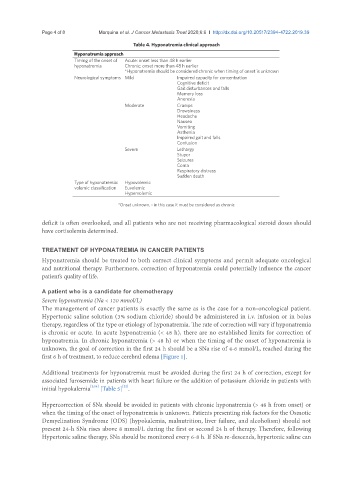
Table 4. Hyponatremia clinical approach
Hyponatremia approach
Timing of the onset of Acute: onset less than 48 h earlier
hyponatremia Chronic: onset more than 48 h earlier
*Hyponatremia should be considered chronic when timing of onset is unknown
Neurological symptoms Mild Impaired capacity for concentration
Cognitive deficit
Gait disturbances and falls
Memory loss
Anorexia
Moderate Cramps
Drowsiness
Headache
Nausea
Vomiting
Asthenia
Impaired gait and falls
Confusion
Severe Lethargy
Stupor
Seizures
Coma
Respiratory distress
Sudden death
Type of hyponatremia: Hypovolemic
volemic classification Euvolemic
Hypervolemic
*Onset unknown, - in this case it must be considered as chronic
deficit is often overlooked, and all patients who are not receiving pharmacological steroid doses should
have cortisolemia determined.
TREATMENT OF HYPONATREMIA IN CANCER PATIENTS
Hyponatremia should be treated to both correct clinical symptoms and permit adequate oncological
and nutritional therapy. Furthermore, correction of hyponatremia could potentially influence the cancer
patient’s quality of life.
A patient who is a candidate for chemotherapy
Severe hyponatremia (Na < 120 mmol/L)
The management of cancer patients is exactly the same as is the case for a non-oncological patient.
Hypertonic saline solution (3% sodium chloride) should be administered in i.v. infusion or in bolus
therapy, regardless of the type or etiology of hyponatremia. The rate of correction will vary if hyponatremia
is chronic or acute. In acute hyponatremia (< 48 h), there are no established limits for correction of
hyponatremia. In chronic hyponatremia (> 48 h) or when the timing of the onset of hyponatremia is
unknown, the goal of correction in the first 24 h should be a SNa rise of 4-6 mmol/L, reached during the
first 6 h of treatment, to reduce cerebral edema [Figure 1].
Additional treatments for hyponatremia must be avoided during the first 24 h of correction, except for
associated furosemide in patients with heart failure or the addition of potassium chloride in patients with
[22]
initial hypokalemia [2,14] [Table 5] .
Hypercorrection of SNa should be avoided in patients with chronic hyponatremia (> 48 h from onset) or
when the timing of the onset of hyponatremia is unknown. Patients presenting risk factors for the Osmotic
Demyelination Syndrome (ODS) (hypokalemia, malnutrition, liver failure, and alcoholism) should not
present 24-h SNa rises above 8 mmol/L during the first or second 24 h of therapy. Therefore, following
Hypertonic saline therapy, SNa should be monitored every 6-8 h. If SNa re-descends, hypertonic saline can