
Page 28 - Read Online
P. 28
De Alcantara Filho et al. J Cancer Metastasis Treat 2019;5:2 I http://dx.doi.org/10.20517/2394-4722.2018.62 Page 3 of 5
A B
Figure 2. A: Intramammary lymph nodes affected by cancer metastases (3/3): capsular extravasation; B: capsular extravasation
A B
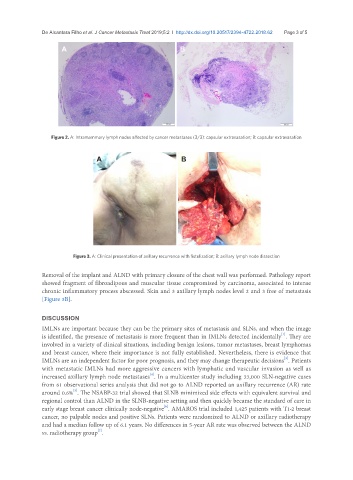
Figure 3. A: Clinical presentation of axillary recurrence with fistulization; B: axillary lymph node dissection
Removal of the implant and ALND with primary closure of the chest wall was performed. Pathology report
showed fragment of fibroadipous and muscular tissue compromised by carcinoma, associated to intense
chronic inflammatory process abscessed. Skin and 3 axillary lymph nodes level 2 and 3 free of metastasis
[Figure 3B].
DISCUSSION
IMLNs are important because they can be the primary sites of metastasis and SLNs, and when the image
[1]
is identified, the presence of metastasis is more frequent than in IMLNs detected incidentally . They are
involved in a variety of clinical situations, including benign lesions, tumor metastases, breast lymphomas
and breast cancer, where their importance is not fully established. Nevertheless, there is evidence that
IMLNs are an independent factor for poor prognosis, and they may change therapeutic decisions . Patients
[3]
with metastatic IMLNs had more aggressive cancers with lymphatic and vascular invasion as well as
increased axillary lymph node metastases . In a multicenter study including 33,000 SLN-negative cases
[4]
from 61 observational series analysis that did not go to ALND reported an axillary recurrence (AR) rate
[5]
around 0.6% . The NSABP-32 trial showed that SLNB minimized side effects with equivalent survival and
regional control than ALND in the SLNB-negative setting and then quickly became the standard of care in
early stage breast cancer clinically node-negative . AMAROS trial included 1,425 patients with T1-2 breast
[6]
cancer, no palpable nodes and positive SLNs. Patients were randomized to ALND or axillary radiotherapy
and had a median follow up of 6.1 years. No differences in 5-year AR rate was observed between the ALND
[7]
vs. radiotherapy group .