
Page 48 - Read Online
P. 48
Page 4 of 9 Sawhney et al. J Cancer Metastasis Treat 2021;7:48 https://dx.doi.org/10.20517/2394-4722.2021.64
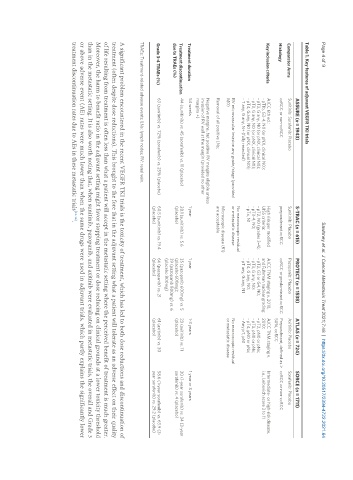
Table 1. Key features of adjuvant VEGFR TKI trials
ASSURE (n = 1943) S-TRAC (n = 615) PROTECT (n = 1538) ATLAS (n = 724) SORCE (n = 1711)
Comparator Arms Sunitinib: Sorafenib: Placebo Sunitinib: Placebo Pazopanib: Placebo Axitinib: Placebo Sorafenib: Placebo
Histology ccRCC or non-ccRCC preponderant ccRCC ccRCC or predominant ccRCC Preponderant, defined as > ccRCC or non-ccRCC
50%, ccRCC
Key inclusion criteria AJCC 6th ed.: High risk per modified AJCC TNM staging v. 2010, AJCC TNM staging v. Intermediate- or high-risk disease,
- pT1b, G3-4, N0 (or pNX, clinical N0); UISS criteria: and Fuhrman nuclear grading: 2010: i.e., Leibovich score 3 to 11
- pT2, G any, N0 (or pNX, clinical N0); - pT2, N0 (grades 3-4); - pT2, G3 or G4, N0; - pT2, pN0 or pNx;
- pT3, G any, N0 (or pNX, clinical N0); - pT3-4, N0; - pT3, G any, N0; - pT3, pN0 or pNx;
- pT4, G any, N0 (or pNX, clinical N0); - pTx, N1 - pT4, G any, N0; - pT4, pN0 or pNx;
- T any, G any, N+ (fully resected) - pT any, G any, N1 - Any pT, pN1
No macroscopic residual
RV microvascular invasion any grade/stage (provided or metastatic disease No macroscopic residual
M0) or metastatic disease
Microscopic disease (R1)
Removal of all positive LNs; are acceptable
Negative margins, but positive RV margins eligible unless
invasion of RV wall at the margin (provided no other
margins +)
Treatment duration 54 weeks 1 year 1 year 1-3 years 1 year or 3 years
Treatment discontinuation 44 (sunitinib) vs. 45 (sorafenib) vs. 11 (placebo) 28.1 (sunitinib) vs. 5.6 35 (pazopanib 600mg) vs. 5 23 (axitinib) vs. 11 30 (1-year sorafenib) vs. 34 (3-year
due to TRAEs (%) (placebo) (placebo 600mg); (placebo) sorafenib) vs. 4 (placebo)
39 (pazopanib 800mg) vs. 6
(placebo 800mg)
Grade 3-4 TRAEs (%) 63 (sunitinib) vs. 72% (sorafenib) vs. 25% (placebo) 60.5 (sunitinib) vs. 19.4 66 (pazopanib) vs. 21 61 (axitinib) vs. 30 58.6 (1-year sorafenib) vs. 63.9 (3-
(placebo) (placebo) (placebo) year sorafenib) vs. 29.2 (placebo)
TRAEs: Treatment-related adverse events; LNs: lymph nodes; RV: renal vein.
A significant problem encountered in the recent VEGFR TKI trials is the toxicity of treatment, which has led to both dose reductions and discontinuation of
treatment (often despite dose reductions). This brought to the fore that in the adjuvant setting what a patient will tolerate as an adverse effect on their quality
of life resulting from treatment is often less than what a patient will accept in the metastatic setting where the perceived benefit of treatment is much greater.
Moreover, the harm to benefit ratio in the adjuvant setting might favor stopping treatment or dose reducing on clinical grounds at a lower toxicity threshold
than in the metastatic setting. It is also worth noting that, when sunitinib, pazopanib, and axitinib were evaluated in metastatic trials, the overall and Grade 3
or above adverse event (AE) rates were much lower than when the same drugs were used in adjuvant trials, which partly explains the significantly lower
treatment discontinuation rates due to AEs in these metastatic trials [13-16] .