
Page 264 - Read Online
P. 264
Chen et al. Hepatoma Res 2019;5:25 I http://dx.doi.org/10.20517/2394-5079.2019.12 Page 5 of 8
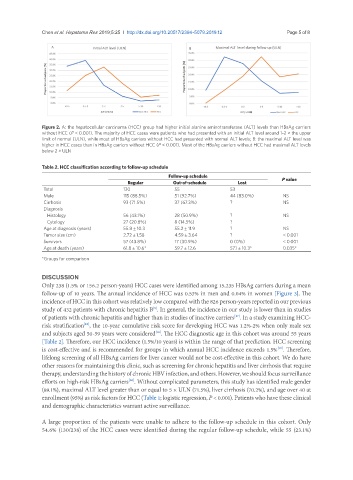
Figure 2. A: the hepatocellular carcinoma (HCC) group had higher initial alanine aminotransferase (ALT) levels than HBsAg carriers
without HCC (P < 0.001). The majority of HCC cases were patients who had presented with an initial ALT level around 1-2 × the upper
limit of normal (ULN), while most of HBsAg carriers without HCC had presented with normal ALT levels; B: the maximal ALT level was
higher in HCC cases than in HBsAg carriers without HCC (P < 0.001). Most of the HBsAg carriers without HCC had maximal ALT levels
below 2 × ULN
Table 2. HCC classification according to follow-up schedule
Follow-up schedule P value
Regular Out-of-schedule Lost
Total 130 55 53
Male 115 (88.5%) 51 (92.7%) 44 (83.0%) NS
Cirrhosis 93 (71.5%) 37 (67.3%) ? NS
Diagnosis
Histology 56 (43.1%) 28 (50.9%) ? NS
Cytology 27 (20.8%) 8 (14.5%) ?
Age at diagnosis (years) 55.8 ± 10.3 55.2 ± 11.9 ? NS
Tumor size (cm) 2.72 ± 1.58 4.59 ± 3.64 ? < 0.001
Survivors 57 (43.8%) 17 (30.9%) 0 (0%) < 0.001
Age at death (years) 61.8 ± 10.6* 59.7 ± 12.6 57.1 ± 10.3* 0.035*
*Groups for comparison
DISCUSSION
Only 238 (1.5% or 156.2 person-years) HCC cases were identified among 15,235 HBsAg carriers during a mean
follow-up of 10 years. The annual incidence of HCC was 0.53% in men and 0.04% in women [Figure 3]. The
incidence of HCC in this cohort was relatively low compared with the 826 person-years reported in our previous
study of 432 patients with chronic hepatitis B . In general, the incidence in our study is lower than in studies
[5]
of patients with chronic hepatitis and higher than in studies of inactive carriers . In a study examining HCC-
[17]
risk stratification , the 10-year cumulative risk score for developing HCC was 1.2%-2% when only male sex
[18]
and subjects aged 50-59 years were considered . The HCC diagnostic age in this cohort was around 55 years
[18]
[Table 2]. Therefore, our HCC incidence (1.5%/10 years) is within the range of that prediction. HCC screening
is cost-effective and is recommended for groups in which annual HCC incidence exceeds 1.5% . Therefore,
[19]
lifelong screening of all HBsAg carriers for liver cancer would not be cost-effective in this cohort. We do have
other reasons for maintaining this clinic, such as screening for chronic hepatitis and liver cirrhosis that require
therapy, understanding the history of chronic HBV infection, and others. However, we should focus surveillance
efforts on high-risk HBsAg carriers . Without complicated parameters, this study has identified male gender
[20]
(89.1%), maximal ALT level greater than or equal to 5 × ULN (71.5%), liver cirrhosis (70.2%), and age over 40 at
enrollment (95%) as risk factors for HCC (Table 1; logistic regression, P < 0.001). Patients who have these clinical
and demographic characteristics warrant active surveillance.
A large proportion of the patients were unable to adhere to the follow-up schedule in this cohort. Only
54.6% (130/238) of the HCC cases were identified during the regular follow-up schedule, while 55 (23.1%)