
Page 228 - Read Online
P. 228
Page 4 of 9 Giorgio et al. Hepatoma Res 2019;5:20 I http://dx.doi.org/10.20517/2394-5079.2019.05
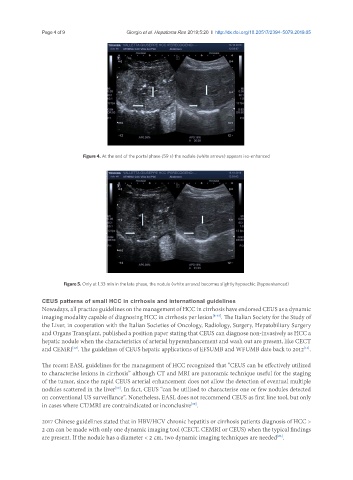
Figure 4. At the end of the portal phase (59 s) the nodule (white arrows) appears iso-enhanced
Figure 5. Only at 1.33 min in the late phase, the nodule (white arrows) becomes slightly hypoechic (hypoenhanced)
CEUS patterns of small HCC in cirrhosis and international guidelines
Nowadays, all practice guidelines on the management of HCC in cirrhosis have endorsed CEUS as a dynamic
imaging modality capable of diagnosing HCC in cirrhosis per lesion [8-13] . The Italian Society for the Study of
the Liver, in cooperation with the Italian Societies of Oncology, Radiology, Surgery, Hepatobiliary Surgery
and Organs Transplant, published a position paper stating that CEUS can diagnose non-invasively as HCC a
hepatic nodule when the characteristics of arterial hyperenhancement and wash out are present, like CECT
and CEMRI . The guidelines of CEUS hepatic applications of EFSUMB and WFUMB date back to 2012 .
[12]
[13]
The recent EASL guidelines for the management of HCC recognized that “CEUS can be effectively utilized
to characterise lesions in cirrhosis” although CT and MRI are panoramic technique useful for the staging
of the tumor, since the rapid CEUS arterial enhancement does not allow the detection of eventual multiple
nodules scattered in the liver . In fact, CEUS “can be utilised to characterise one or few nodules detected
[10]
on conventional US surveillance”. Nonetheless, EASL does not recommend CEUS as first line tool, but only
in cases where CT/MRI are contraindicated or inconclusive .
[10]
2017 Chinese guidelines stated that in HBV/HCV chronic hepatitis or cirrhosis patients diagnosis of HCC >
2 cm can be made with only one dynamic imaging tool (CECT, CEMRI or CEUS) when the typical findings
are present. If the nodule has a diameter < 2 cm, two dynamic imaging techniques are needed .
[23]