
Page 175 - Read Online
P. 175
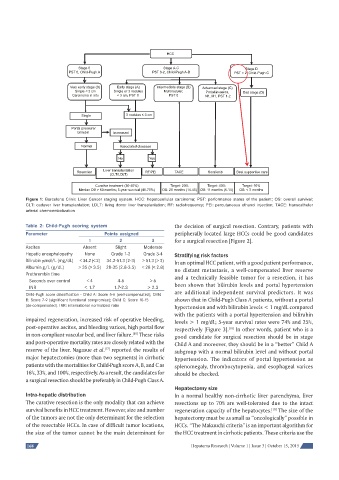
HCC
Stage 0 Stage A-C Stage D
PST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST > 2, Child-Pugh C
Very early stage (0) Early stage (A) Intermediate stage (B) Advanced stage (C)
Single < 2 cm Single or 3 nodules Multinodular, Portal invasion, End stage (D)
Carcinoma in situ < 3 cm, PST 0 PST 0 N1, M1, PST 1-2
Single 3 nodules ≤ 3 cm
Portal pressure/
bilirubin Increased
Normal Associated diseases
No Yes
Liver transplantation
Resection RF/PEI TACE Sorafenib Best supportive care
(CLT/LDLT)
Curative treatment (30-40%) Target: 20% Target: 40% Target: 10%
Median OS > 60 months; 5-year survival (40-70%) OS: 20 months (14-45) OS: 11 months (6-14) OS: < 3 months
Figure 1: Barcelona Clinic Liver Cancer staging system. HCC: hepatocellular carcinoma; PST: performance status of the patient; OS: overall survival;
CLT: cadaver liver transplantation; LDLT: living donor liver transplantation; RF: radiofrequency; PEI: percutaneous ethanol injection; TACE: transcatheter
arterial chemoembolization
Table 2: Child-Pugh scoring system the decision of surgical resection. Contrary, patients with
Parameter Points assigned peripherally located large HCCs could be good candidates
1 2 3 for a surgical resection [Figure 2].
Ascites Absent Slight Moderate
Hepatic encephalopathy None Grade 1-2 Grade 3-4 Stratifying risk factors
Bilirubin μmol/L (mg/dL) < 34.2 (< 2) 34.2-51.3 (2-3) > 51.3 (> 3) In an optimal HCC patient, with a good patient performance,
Albumin g/L (g/dL) > 35 (> 3.5) 28-35 (2.8-3.5) < 28 (< 2.8)
no distant metastasis, a well-compensated liver reserve
Prothrombin time
and a technically feasible tumor for a resection, it has
Seconds over control < 4 4-6 > 6
been shown that bilirubin levels and portal hypertension
INR < 1.7 1.7-2.3 > 2.3
are additional independent survival predictors. It was
Child-Pugh score classifi cation - Child A: Score 5-6 (well-compensated); Child
shown that in Child-Pugh Class A patients, without a portal
B: Score 7-9 (signifi cant functional compromise); Child C: Score 10-15
(de-compensated). INR: international normalized ratio hypertension and with bilirubin levels < 1 mg/dL compared
with the patients with a portal hypertension and bilirubin
impaired regeneration, increased risk of operative bleeding, levels > 1 mg/dL; 5-year survival rates were 74% and 25%,
post-operative ascites, and bleeding varices, high portal flow respectively [Figure 3]. In other words, patient who is a
[18]
in non-compliant vascular bed, and liver failure. These risks good candidate for surgical resection should be in stage
[16]
and post-operative mortality rates are closely related with the Child A and moreover, they should be in a “better” Child A
[17]
reserve of the liver. Nagasue et al. reported the results of subgroup with a normal bilirubin level and without portal
major hepatectomies (more than two segments) in cirrhotic hypertension. The indicators of portal hypertension as
patients with the mortalities for Child-Pugh score A, B, and C as splenomegaly, thrombocytopenia, and esophageal varices
16%, 33%, and 100%, respectively. As a result, the candidates for should be checked.
a surgical resection should be preferably in Child-Pugh Class A.
Hepatectomy size
Intra-hepatic distribution In a normal healthy non-cirrhotic liver parenchyma, liver
The curative resection is the only modality that can achieve resections up to 70% are well-tolerated due to the intact
survival benefits in HCC treatment. However, size and number regeneration capacity of the hepatocytes. The size of the
[19]
of the tumors are not the only determinant for the selection hepatectomy must be as small as “oncologically” possible in
of the resectable HCCs. In case of difficult tumor locations, HCCs. “The Makuuchi criteria” is an important algorithm for
the size of the tumor cannot be the main determinant for the HCC treatment in cirrhotic patients. These criteria use the
168 Hepatoma Research | Volume 1 | Issue 3 | October 15, 2015