
Page 36 - Read Online
P. 36
Mathias-Machado et al. Hepatoma Res 2021;7:67 https://dx.doi.org/10.20517/2394-5079.2021.84 Page 9 of 12
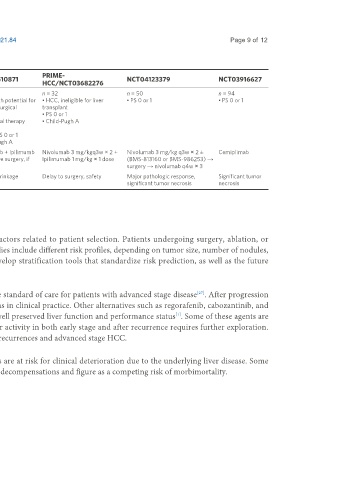
Table 2. Main ongoing studies with immune checkpoint inhibitors in the neoadjuvant setting
PRIME-
NCT03222076 AURORA/NCT03337841 NCT03510871 NCT04123379 NCT03916627
HCC/NCT03682276
Patient n = 45 n = 50 n = 40 n = 32 n = 50 n = 94
population • Prior therapy allowed, including • Child-Pugh A • HCC with potential for • HCC, ineligible for liver • PS 0 or 1 • PS 0 or 1
surgery, RT, LRT, and systemic • PS 0 curative surgical transplant
therapy (sorafenib and resection • PS 0 or 1
chemotherapy) • Prior local therapy • Child-Pugh A
• PS ≤ 1 allowed
• ECOG PS 0 or 1
• Child-Pugh A
Treatment Nivolumab q2w ± ipililumab q2w × 3 Pembrolizumb 200 mg × 1 dose → Nivolumab + Ipilimumb Nivolumab 3 mg/kgq3w × 2 + Nivolumab 3 mg/kg q3w × 2 ± Cemiplimab
doses → liver surgery → nivolumab resection or RFA → Pembrolizumb 200 → curative surgery, if Ipilimumab 1 mg/kg × 1 dose (BMS-813160 or BMS-986253) →
q4w ± ipililumab q6w mg q3w eligible surgery → nivolumab q4w × 3
Primary Safety 1-year RFS Tumor shrinkage Delay to surgery, safety Major pathologic response, Significant tumor
endpoint(s) significant tumor necrosis necrosis
RT: Radiotherapy; LRT: locoregional therapies; PS: performance status; RFA: radiofrequency ablation.
CHALLENGES IN TRIAL DESIGN
The interpretation of adjuvant studies for HCC is complex due to several factors related to patient selection. Patients undergoing surgery, ablation, or
transplantation have different risk stratifications for recurrence. In general, studies include different risk profiles, depending on tumor size, number of nodules,
histological differentiation, and microvascular invasion. It is necessary to develop stratification tools that standardize risk prediction, as well as the future
incorporation of tools for molecular tumor characterization.
Atezolizumab (anti-PD-L1) plus bevacizumab (anti-VEGF) combination is the standard of care for patients with advanced stage disease . After progression
[27]
to first line, TKIs such as sorafenib and lenvatinib are the most adopted options in clinical practice. Other alternatives such as regorafenib, cabozantinib, and
ramucirumab are reasonable choices in later lines, whenever patients present well preserved liver function and performance status . Some of these agents are
[1]
being tested in the (neo)adjuvant setting. Whether these drugs will retain their activity in both early stage and after recurrence requires further exploration.
Positive results in these trials would influence decision making on how to treat recurrences and advanced stage HCC.
Finally, safety is a key challenge for clinical trials in early stages. HCC patients are at risk for clinical deterioration due to the underlying liver disease. Some
drugs are associated with treatment-related adverse events that can lead to liver decompensations and figure as a competing risk of morbimortality.