
Page 151 - Read Online
P. 151
Ghunaim et al. Vessel Plus 2023;7:29 https://dx.doi.org/10.20517/2574-1209.2023.112 Page 5 of 17
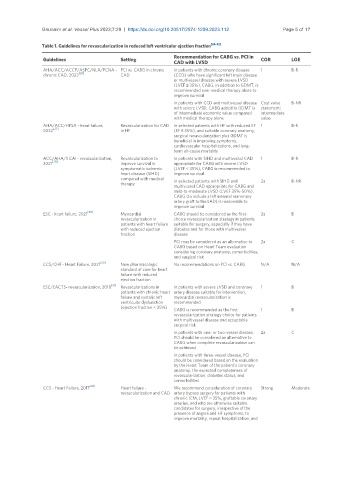
Table 1. Guidelines for revascularization in reduced left ventricular ejection fraction [26-32]
Recommendation for CABG vs. PCI in
Guidelines Setting COR LOE
CAD with LVSD
AHA/ACC/ACCP/ASPC/NLA/PCNA - PCI vs. CABG in chronic In patients with chronic coronary disease 1 B-R
chronic CAD, 2023 [26] CAD (CCD) who have significant left main disease
or multivessel disease with severe LVSD
(LVEF ≤ 35%), CABG, in addition to GDMT, is
recommended over medical therapy alone to
improve survival
In patients with CCD and multivessel disease Cost value B-NR
with severe LVSD, CABG added to GDMT is statement:
of intermediate economic value compared intermediate
with medical therapy alone value
AHA/ACC/HFSA - heart failure, Revascularization for CAD In selected patients with HF with reduced EF 1 B-R
[27]
2022 in HF (EF ≤ 35%), and suitable coronary anatomy,
surgical revascularization plus GDMT is
beneficial in improving symptoms,
cardiovascular hospitalizations, and long-
term all-cause mortality
ACC/AHA/S CAI - revascularization, Revascularization to In patients with SIHD and multivessel CAD 1 B-R
2021 [28] improve survival in appropriate for CABG with severe LVSD
symptomatic ischemic (LVEF < 35%), CABG is recommended to
heart disease (SIHD) improve survival
compared with medical In selected patients with SIHD and 2a B-NR
therapy
multivessel CAD appropriate for CABG and
mild-to-moderate LVSD (LVEF 35%-50%),
CABG (to include a left internal mammary
artery graft to the LAD) is reasonable to
improve survival
ESC - heart failure, 2021 [29] Myocardial CABG should be considered as the first- 2a B
revascularization in choice revascularization strategy in patients
patients with heart failure suitable for surgery, especially if they have
with reduced ejection diabetes and for those with multivessel
fraction disease
PCI may be considered as an alternative to 2a C
CABG based on Heart Team evaluation
considering coronary anatomy, comorbidities,
and surgical risk
[30]
CCS/CHF - Heart Failure, 2021 New pharmacologic No recommendations on PCI vs. CABG N/A N/A
standard of care for heart
failure with reduced
ejection fraction
ESC/EACTS- revascularization, 2018 [31] Revascularizations in In patients with severe LVSD and coronary 1 B
patients with chronic heart artery disease suitable for intervention,
failure and systolic left myocardial revascularization is
ventricular dysfunction recommended
(ejection fraction < 35%)
CABG is recommended as the first 1 B
revascularization strategy choice for patients
with multivessel disease and acceptable
surgical risk
In patients with one- or two-vessel disease, 2a C
PCI should be considered an alternative to
CABG when complete revascularization can
be achieved
In patients with three-vessel disease, PCI
should be considered based on the evaluation
by the Heart Team of the patient’s coronary
anatomy, the expected completeness of
revascularization, diabetes status, and
comorbidities
[32]
CCS - Heart Failure, 2017 Heart failure - We recommend consideration of coronary Strong Moderate
revascularization and CAD artery bypass surgery for patients with
chronic ICM, LVEF < 35%, graftable coronary
arteries, and who are otherwise suitable
candidates for surgery, irrespective of the
presence of angina and HF symptoms, to
improve mortality, repeat hospitalization, and