
Page 650 - Read Online
P. 650
Page 6 of 13 Theisen et al. Plast Aesthet Res 2020;7:56 I http://dx.doi.org/10.20517/2347-9264.2020.83
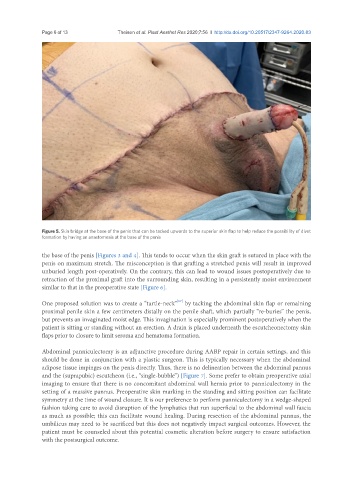
Figure 5. Skin bridge at the base of the penis that can be tacked upwards to the superior skin flap to help reduce the possibility of divot
formation by having an anastomosis at the base of the penis
the base of the penis [Figures 3 and 4]. This tends to occur when the skin graft is sutured in place with the
penis on maximum stretch. The misconception is that grafting a stretched penis will result in improved
unburied length post-operatively. On the contrary, this can lead to wound issues postoperatively due to
retraction of the proximal graft into the surrounding skin, resulting in a persistently moist environment
similar to that in the preoperative state [Figure 6].
[17]
One proposed solution was to create a “turtle-neck” by tacking the abdominal skin flap or remaining
proximal penile skin a few centimeters distally on the penile shaft, which partially “re-buries” the penis,
but prevents an invaginated moist edge. This invagination is especially prominent postoperatively when the
patient is sitting or standing without an erection. A drain is placed underneath the escutcheonectomy skin
flaps prior to closure to limit seroma and hematoma formation.
Abdominal panniculectomy is an adjunctive procedure during AABP repair in certain settings, and this
should be done in conjunction with a plastic surgeon. This is typically necessary when the abdominal
adipose tissue impinges on the penis directly. Thus, there is no delineation between the abdominal pannus
and the (suprapubic) escutcheon (i.e., “single-bubble”) [Figure 7]. Some prefer to obtain preoperative axial
imaging to ensure that there is no concomitant abdominal wall hernia prior to panniculectomy in the
setting of a massive pannus. Preoperative skin marking in the standing and sitting position can facilitate
symmetry at the time of wound closure. It is our preference to perform panniculectomy in a wedge-shaped
fashion taking care to avoid disruption of the lymphatics that run superficial to the abdominal wall fascia
as much as possible; this can facilitate wound healing. During resection of the abdominal pannus, the
umbilicus may need to be sacrificed but this does not negatively impact surgical outcomes. However, the
patient must be counseled about this potential cosmetic alteration before surgery to ensure satisfaction
with the postsurgical outcome.