
Page 442 - Read Online
P. 442
Lemperle Plast Aesthet Res 2020;7:40 I http://dx.doi.org/10.20517/2347-9264.2020.14 Page 11 of 25
A B
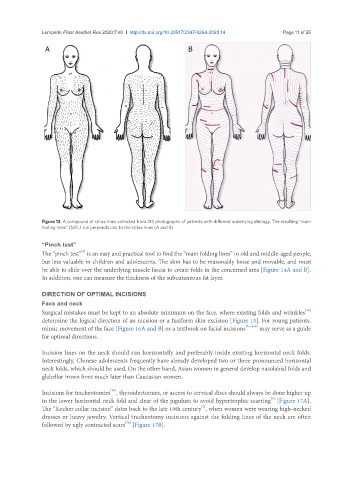
Figure 13. A compound of striae lines collected from 213 photographs of patients with different underlying etiology. The resulting “main
folding lines” (MFL) run perpendicular to the striae lines (A and B)
“Pinch test”
[3]
The “pinch test” is an easy and practical tool to find the “main folding lines” in old and middle-aged people,
but less valuable in children and adolescents. The skin has to be reasonably loose and movable, and must
be able to slide over the underlying muscle fascia to create folds in the concerned area [Figure 14A and B].
In addition, one can measure the thickness of the subcutaneous fat layer.
DIRECTION OF OPTIMAL INCISIONS
Face and neck
[36]
Surgical mistakes must be kept to an absolute minimum on the face, where existing folds and wrinkles
determine the logical direction of an incision or a fusiform skin excision [Figure 15]. For young patients,
mimic movement of the face [Figure 16A and B] or a textbook on facial incisions [2,4,6-8] may serve as a guide
for optimal directions.
Incision lines on the neck should run horizontally and preferably inside existing horizontal neck folds.
Interestingly, Chinese adolescents frequently have already developed two or three pronounced horizontal
neck folds, which should be used. On the other hand, Asian women in general develop nasolabial folds and
glabellar frown lines much later than Caucasian women.
Incisions for tracheotomies , thyroidectomies, or access to cervical discs should always be done higher up
[36]
[5]
in the lower horizontal neck fold and clear of the jugulum to avoid hypertrophic scarring [Figure 17A].
[2]
The “Kocher collar incision” dates back to the late 19th century , when women were wearing high-necked
dresses or heavy jewelry. Vertical tracheotomy incisions against the folding lines of the neck are often
followed by ugly contracted scars [Figure 17B].
[36]