
Page 13 - Read Online
P. 13
Shaw et al. Plast Aesthet Res 2021;8:52 https://dx.doi.org/10.20517/2347-9264.2021.53 Page 7 of 11
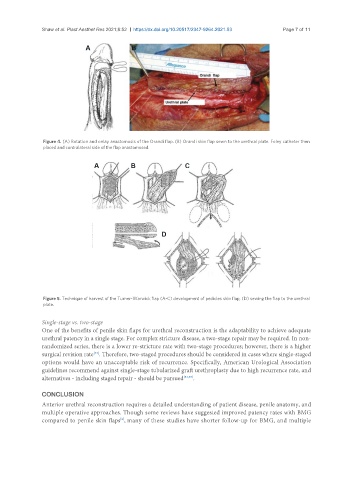
Figure 4. (A) Rotation and onlay anastomosis of the Orandi flap. (B) Orandi skin flap sewn to the urethral plate. Foley catheter then
placed and contralateral side of the flap anastomosed.
Figure 5. Technique of harvest of the Turner-Warwick flap (A-C) development of pedicles skin flap, (D) sewing the flap to the urethral
plate.
Single-stage vs. two-stage
One of the benefits of penile skin flaps for urethral reconstruction is the adaptability to achieve adequate
urethral patency in a single stage. For complex stricture disease, a two-stage repair may be required. In non-
randomized series, there is a lower re-stricture rate with two-stage procedures; however, there is a higher
[33]
surgical revision rate . Therefore, two-staged procedures should be considered in cases where single-staged
options would have an unacceptable risk of recurrence. Specifically, American Urological Association
guidelines recommend against single-stage tubularized graft urethroplasty due to high recurrence rate, and
alternatives - including staged repair - should be pursued [34,35] .
CONCLUSION
Anterior urethral reconstruction requires a detailed understanding of patient disease, penile anatomy, and
multiple operative approaches. Though some reviews have suggested improved patency rates with BMG
[8]
compared to penile skin flaps , many of these studies have shorter follow-up for BMG, and multiple