
Page 59 - Read Online
P. 59
Lies et al. Plast Aesthet Res 2019;6:18 I http://dx.doi.org/10.20517/2347-9264.2019.27 Page 5 of 9
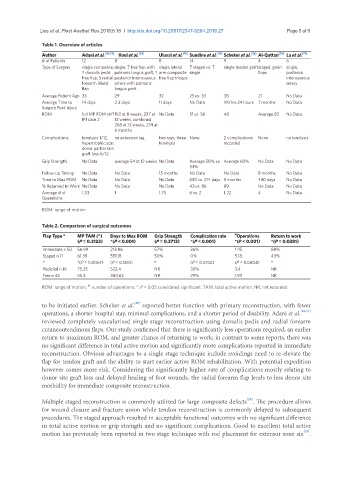
Table 1. Overview of articles
Author Adani et al. [26,27] Koul et al. [33] Ulusal et al. [19] Sundine et al. [24] Scheker et al. [25] Al-Qattan [29] Lu et al. [17]
# of Patients 12 8 8 14 9 4 6
Type of Surgery single composite, single, 7 free flap with single lateral 7 staged vs. 7 single tendon graftstaged, groin single,
7 dorsalis pedis palmaris longus graft, 1 arm composite single flaps posterior
free flap, 5 radial posterior interosseous free flap triceps interosseous
forearm island artery with palmaris artery
flap longus graft
Average Patient Age 33 29 32 25 vs. 33 38 21 No Data
Average Time to 14 days 2.3 days 11 days No Data Within 24 hours 7 months No Data
Surgery Post-Injury
ROM full MP ROM stiff 192 at 8 weeks, 237 at No Data 51 vs. 56 48 Average 82 No Data
IPJ case 2 12 weeks, combined
268 at 12 weeks, 274 at
6 months
Complications tenolysis 1/12, no extension lag two rays, three None 2 complications None no tenolysis
hypertrophic scar, tenolysis recorded
donor partial skin
graft loss 6/12
Grip Strength No Data average 54 at 12 weeks No Data Average 50% vs. Average 60% No Data No Data
53%
Follow-up Timing No Data No Data 15 months No Data No Data 8 months No Data
Time to Max ROM No Data No Data No Data 630 vs. 214 days 3 months 430 days No Data
% Returned to Work No Data No Data No Data 43 vs. 86 89 No Data No Data
Average # of 1.33 1 1.75 6 vs. 2 1.22 4 No Data
Operations
ROM: range of motion
Table 2. Comparison of surgical outcomes
Flap Type ° MP TAM (°) Days to Max ROM Grip Strength Complication rate # Operations Return to work
(P = 0.3123) *(P < 0.001) (P = 0.2713) *(P < 0.001) *(P < 0.001) *(P = 0.0381)
Immediate n 50 56.99 213.86 57% 36% 1.45 88%
Staged n 11 61.39 551.18 50% 0% 5.18 43%
° *(P = 0.0067) (P = 0.1610) ° (P = 0.4740) (P = 0.0604) °
Pedicled n 16 75.25 522.4 NR 30% 3.4 NR
Free n 45 55.4 380.62 NR 29% 1.93 NR
ROM: range of motion; : number of operations; *: P < 0.05 considered significant; TAM: total active motion; NR: not recorded
#
to be initiated earlier. Scheker et al. reported better function with primary reconstruction, with fewer
[25]
operations, a shorter hospital stay, minimal complications, and a shorter period of disability. Adani et al. [26,27]
reviewed completely vascularized single stage reconstruction using dorsalis pedis and radial forearm
cutaneoutendinous flaps. Our study confirmed that there is significantly less operations required, an earlier
return to maximum ROM, and greater chance of returning to work; in contrast to some reports, there was
no significant difference in total active motion and significantly more complications reported in immediate
reconstruction. Obvious advantages to a single stage technique include avoidings need to re-elevate the
flap for tendon graft and the ability to start earlier active ROM rehabilitation. With potential expedition
however comes more risk. Considering the significantly higher rate of complications mostly relating to
donor site graft loss and delayed healing of foot wounds, the radial forearm flap lends to less donor site
morbidity for immediate composite reconstruction.
Multiple staged reconstruction is commonly utilized for large composite defects . The procedure allows
[28]
for wound closure and fracture union while tendon reconstruction is commonly delayed to subsequent
procedures. The staged approach resulted in acceptable functional outcomes with no significant difference
in total active motion or grip strength and no significant complications. Good to excellent total active
[29]
motion has previously been reported in two stage technique with rod placement for extensor zone six .