
Page 221 - Read Online
P. 221
Page 10 of 13 Climent et al. Mini-invasive Surg 2018;2:45 I http://dx.doi.org/10.20517/2574-1225.2018.62
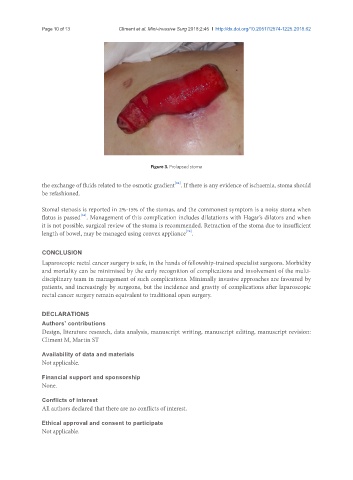
Figure 3. Prolapsed stoma
[64]
the exchange of fluids related to the osmotic gradient . If there is any evidence of ischaemia, stoma should
be refashioned.
Stomal stenosis is reported in 2%-15% of the stomas, and the commonest symptom is a noisy stoma when
[64]
flatus is passed . Management of this complication includes dilatations with Hagar’s dilators and when
it is not possible, surgical review of the stoma is recommended. Retraction of the stoma due to insufficient
[75]
length of bowel, may be managed using convex appliance .
CONCLUSION
Laparoscopic rectal cancer surgery is safe, in the hands of fellowship-trained specialist surgeons. Morbidity
and mortality can be minimised by the early recognition of complications and involvement of the multi-
disciplinary team in management of such complications. Minimally invasive approaches are favoured by
patients, and increasingly by surgeons, but the incidence and gravity of complications after laparoscopic
rectal cancer surgery remain equivalent to traditional open surgery.
DECLARATIONS
Authors’ contributions
Design, literature research, data analysis, manuscript writing, manuscript editing, manuscript revision:
Climent M, Martin ST
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.