
Page 22 - Read Online
P. 22
Page 4 of 11 Vong et al. J Cancer Metastasis Treat 2020;6:54 I http://dx.doi.org/10.20517/2394-4722.2020.116
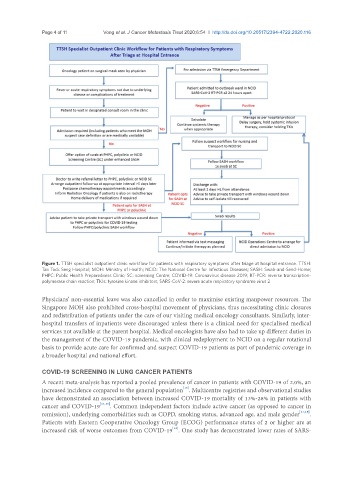
Figure 1. TTSH specialist outpatient clinic workflow for patients with respiratory symptoms after triage at hospital entrance. TTSH:
Tan Tock Seng Hospital; MOH: Ministry of Health; NCID: The National Centre for Infectious Diseases; SASH: Swab-and-Send-Home;
PHPC: Public Health Preparedness Clinic; SC: screening Centre; COVID-19: Coronavirus disease 2019; RT-PCR: reverse transcription-
polymerase chain reaction; TKIs: tyrosine kinase inhibitors; SARS-CoV-2: severe acute respiratory syndrome virus 2
Physicians’ non-essential leave was also cancelled in order to maximise existing manpower resources. The
Singapore MOH also prohibited cross-hospital movement of physicians, thus necessitating clinic closures
and redistribution of patients under the care of our visiting medical oncology consultants. Similarly, inter-
hospital transfers of inpatients were discouraged unless there is a clinical need for specialised medical
services not available at the parent hospital. Medical oncologists have also had to take up different duties in
the management of the COVID-19 pandemic, with clinical redeployment to NCID on a regular rotational
basis to provide acute care for confirmed and suspect COVID-19 patients as part of pandemic coverage in
a broader hospital and national effort.
COVID-19 SCREENING IN LUNG CANCER PATIENTS
A recent meta-analysis has reported a pooled prevalence of cancer in patients with COVID-19 of 2.0%, an
[13]
increased incidence compared to the general population . Multicentre registries and observational studies
have demonstrated an association between increased COVID-19 mortality of 13%-28% in patients with
cancer and COVID-19 [14,15] . Common independent factors include active cancer (as opposed to cancer in
remission), underlying comorbidities such as COPD, smoking status, advanced age, and male gender [14,15] .
Patients with Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher are at
[14]
increased risk of worse outcomes from COVID-19 . One study has demonstrated lower rates of SARS-