
Page 39 - Read Online
P. 39
Berardi et al. J Cancer Metastasis Treat 2019;5:79 I http://dx.doi.org/10.20517/2394-4722.2019.008 Page 7 of 33
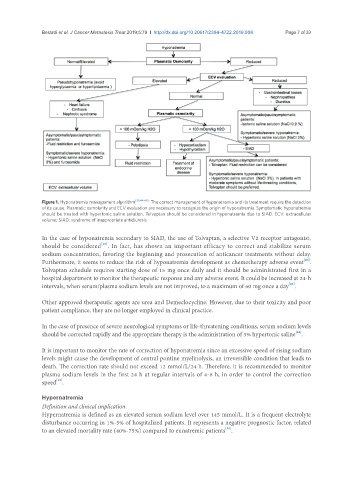
Figure 1. Hyponatremia management algorithm [38,44-48] . The correct management of hyponatremia and its treatment require the detection
of its cause. Plasmatic osmolarity and ECV evaluation are necessary to recognize the origin of hyponatremia. Symptomatic hyponatremia
should be treated with hypertonic saline solution. Tolvaptan should be considered in hyponatremia due to SIAD. ECV: extracellular
volume; SIAD: syndrome of inappropriate antidiuresis
In the case of hyponatremia secondary to SIAD, the use of Tolvaptan, a selective V2 receptor antagonist,
[46]
should be considered . In fact, has shown an important efficacy to correct and stabilize serum
sodium concentration, favoring the beginning and prosecution of anticancer treatments without delay.
[47]
Furthermore, it seems to reduce the risk of hyponatremia development as chemotherapy adverse event .
Tolvaptan schedule requires starting dose of 15 mg once daily and it should be administrated first in a
hospital department to monitor the therapeutic response and any adverse event. It could be increased at 24-h
[46]
intervals, when serum/plasma sodium levels are not improved, to a maximum of 60 mg once a day .
Other approved therapeutic agents are urea and Demeclocycline. However, due to their toxicity and poor
patient compliance, they are no longer employed in clinical practice.
In the case of presence of severe neurological symptoms or life-threatening conditions, serum sodium levels
[48]
should be corrected rapidly and the appropriate therapy is the administration of 3% hypertonic saline .
It is important to monitor the rate of correction of hyponatremia since an excessive speed of rising sodium
levels might cause the development of central pontine myelinolysis, an irreversible condition that leads to
death. The correction rate should not exceed 12 mmol/L/24 h. Therefore, it is recommended to monitor
plasma sodium levels in the first 24 h at regular intervals of 4-6 h, in order to control the correction
[49]
speed .
Hypernatremia
Definition and clinical implication
Hypernatremia is defined as an elevated serum sodium level over 145 mmol/L. It is a frequent electrolyte
disturbance occurring in 1%-5% of hospitalized patients. It represents a negative prognostic factor, related
[50]
to an elevated mortality rate (40%-75%) compared to eunatremic patients .