
Page 141 - Read Online
P. 141
Page 2 of 12 Kamiya et al. J Cancer Metastasis Treat 2018;4:35 I http://dx.doi.org/10.20517/2394-4722.2017.76
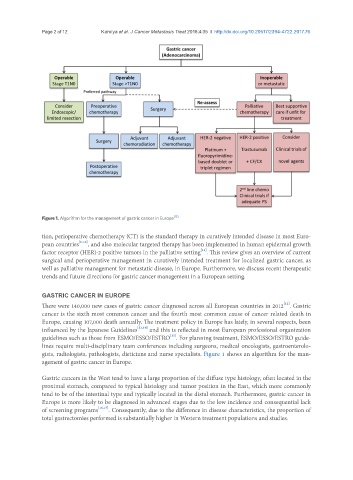
Figure 1. Algorithm for the management of gastric cancer in Europe [15]
tion, perioperative chemotherapy (CT) is the standard therapy in curatively intended disease in most Euro-
pean countries [6-10] , and also molecular targeted therapy has been implemented in human epidermal growth
[11]
factor receptor (HER)-2 positive tumors in the palliative setting . This review gives an overview of current
surgical and perioperative management in curatively intended treatment for localized gastric cancer, as
well as palliative management for metastatic disease, in Europe. Furthermore, we discuss recent therapeutic
trends and future directions for gastric cancer management in a European setting.
GASTRIC CANCER IN EUROPE
[12]
There were 140,000 new cases of gastric cancer diagnosed across all European countries in 2012 . Gastric
cancer is the sixth most common cancer and the fourth most common cause of cancer related death in
Europe, causing 107,000 death annually. The treatment policy in Europe has lately, in several respects, been
influenced by the Japanese Guidelines [13,14] and this is reflected in most European professional organization
[15]
guidelines such as those from ESMO/ESSO/ESTRO . For planning treatment, ESMO/ESSO/ESTRO guide-
lines require multi-disciplinary team conferences including surgeons, medical oncologists, gastroenterolo-
gists, radiologists, pathologists, dieticians and nurse specialists. Figure 1 shows an algorithm for the man-
agement of gastric cancer in Europe.
Gastric cancers in the West tend to have a large proportion of the diffuse type histology, often located in the
proximal stomach, compared to typical histology and tumor position in the East, which more commonly
tend to be of the intestinal type and typically located in the distal stomach. Furthermore, gastric cancer in
Europe is more likely to be diagnosed in advanced stages due to the low incidence and consequential lack
of screening programs [16,17] . Consequently, due to the difference in disease characteristics, the proportion of
total gastrectomies performed is substantially higher in Western treatment populations and studies.