
Page 830 - Read Online
P. 830
Bhangui et al. Hepatoma Res 2020;6:71 I http://dx.doi.org/10.20517/2394-5079.2020.67 Page 9 of 15
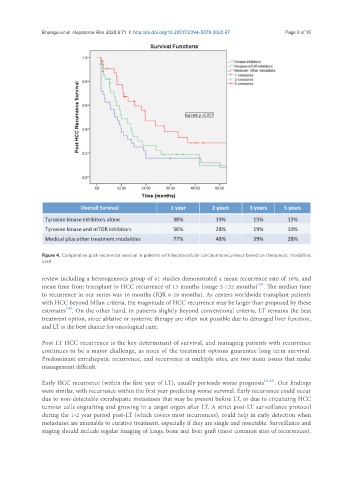
Figure 4. Comparative post-recurrence survival in patients with hepatocellular carcinoma recurrence based on therapeutic modalities
used
review including a heterogeneous group of 61 studies demonstrated a mean recurrence rate of 16%, and
[19]
mean time from transplant to HCC recurrence of 13 months (range 2-132 months) . The median time
to recurrence in our series was 16 months (IQR 8-29 months). As centers worldwide transplant patients
with HCC beyond Milan criteria, the magnitude of HCC recurrence may be larger than proposed by these
[20]
estimates . On the other hand, in patients slightly beyond conventional criteria, LT remains the best
treatment option, since ablative or systemic therapy are often not possible due to deranged liver function,
and LT is the best chance for oncological cure.
Post LT HCC recurrence is the key determinant of survival, and managing patients with recurrence
continues to be a major challenge, as none of the treatment options guarantee long term survival.
Predominant extrahepatic recurrence, and recurrence at multiple sites, are two main issues that make
management difficult.
Early HCC recurrence (within the first year of LT), usually portends worse prognosis [21,22] . Our findings
were similar, with recurrence within the first year predicting worse survival. Early recurrence could occur
due to non-detectable extrahepatic metastases that may be present before LT, or due to circulating HCC
tumour cells engrafting and growing in a target organ after LT. A strict post-LT surveillance protocol
during the 1-2 year period post-LT (which covers most recurrences), could help in early detection when
metastases are amenable to curative treatment, especially if they are single and resectable. Surveillance and
staging should include regular imaging of lungs, bone and liver graft (most common sites of recurrences),