
Page 86 - Read Online
P. 86
Pazgan-Simon. Hepatoma Res 2020;6:17 I http://dx.doi.org/10.20517/2394-5079.2019.52 Page 5 of 8
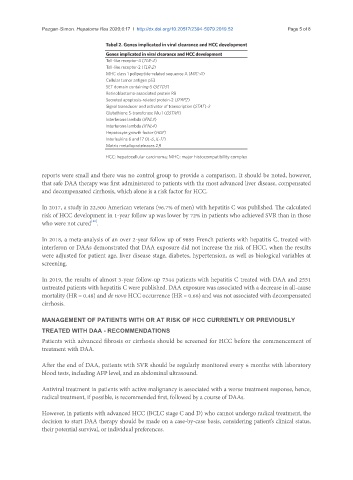
Tabel 2. Genes implicated in viral clearance and HCC development
Genes implicated in viral clearance and HCC development
Toll-like receptor-4 (TLR-4)
Toll-like receptor-2 (TLR-2)
MHC class 1 polipeptide-related sequence A (MIC-A)
Cellular tumor antigen p53
SET domain containing-5 (SETD5)
Retinoblastoma-associated protein RB
Secreted apoptosis-related protein-2 (SFRP2)
Signal transducer and activator of transcription (STAT)-3
Glutathione S-transferase Mu 1 (GSTM1)
Interferone lambda (IFNL3)
Interferone lambda (IFNL4)
Hepatocyte growth factor (HGF)
Interleukins 6 and 17 (IL-6, IL-17)
Matrix metalloproteinases 2,9
HCC: hepatocellular carcinoma; MHC: major histocompatibility complex
reports were small and there was no control group to provide a comparison. It should be noted, however,
that safe DAA therapy was first administered to patients with the most advanced liver disease, compensated
and decompensated cirrhosis, which alone is a risk factor for HCC.
In 2017, a study in 22,500 American veterans (96.7% of men) with hepatitis C was published. The calculated
risk of HCC development in 1-year follow up was lower by 72% in patients who achieved SVR than in those
[11]
who were not cured .
In 2018, a meta-analysis of an over 2-year follow up of 9895 French patients with hepatitis C, treated with
interferon or DAAs demonstrated that DAA exposure did not increase the risk of HCC, when the results
were adjusted for patient age, liver disease stage, diabetes, hypertension, as well as biological variables at
screening.
In 2019, the results of almost 3-year follow-up 7344 patients with hepatitis C treated with DAA and 2551
untreated patients with hepatitis C were published. DAA exposure was associated with a decrease in all-cause
mortality (HR = 0.48) and de novo HCC occurrence (HR = 0.66) and was not associated with decompensated
cirrhosis.
MANAGEMENT OF PATIENTS WITH OR AT RISK OF HCC CURRENTLY OR PREVIOUSLY
TREATED WITH DAA - RECOMMENDATIONS
Patients with advanced fibrosis or cirrhosis should be screened for HCC before the commencement of
treatment with DAA.
After the end of DAA, patients with SVR should be regularly monitored every 6 months with laboratory
blood tests, including AFP level, and an abdominal ultrasound.
Antiviral treatment in patients with active malignancy is associated with a worse treatment response, hence,
radical treatment, if possible, is recommended first, followed by a course of DAAs.
However, in patients with advanced HCC (BCLC stage C and D) who cannot undergo radical treatment, the
decision to start DAA therapy should be made on a case-by-case basis, considering patient’s clinical status,
their potential survival, or individual preferences.